![Room9er ["Room Niner"]:](https://room9er.com/wp-content/uploads/2020/03/cropped-Screen-Shot-2020-03-08-at-3.16.16-PM.png)
Here is a practical YouTube video on performing physical examination of the hand. Courtesy of Dr Mallory.
Post-Publication Peer Review
For those who have not been introduced to this concept, here is a blog post from Dr Radecki who writes the EM Lit of Note.
Because blog posts are not “peer-reviewed” before they are posted, the quality of a given post could be low. But depending on how many people read the post, the discussion can be lively and constructive.
This is in contrast to formal journal publication, where the peer review is PRE-publication, and discussion may be minimal. We will see a comment or two in an issue a month or two later, sometimes an official comment in the same issue. But the volume and even quality of responses possible with blogs, twitter, etc may surpass that of the official, slow process in the journals.
Scientific American had a nice article about this PPPR concept. As FOAMed and social media continues to expand in medicine, and in other fields, I think we will see more respect for this type of peer-review.
Journal Club May 2014
Journal Club is this coming Thursday, May 22.
Where:
Kashmir Indian Restaurant (Patio!) (Beer + wine!) (I absolutely love this place.)
1285 Bardstown Road
(loads of parking across the street in the Mid City Mall)
When:
7 PM
Email or text me if you will be there.
Attached articles:
1. Hypnosis in the ED
2. Wound management myths
3. Is it actually a spider bite?
Routine Coags in Chest Pain
Thought this was a great little post regarding Coagulation studies in chest pain patients. Not sure how often its getting routinely obtained on our CP patients @ UofL but at Norton they get it on almost every chest pain patient that rolls through the door.
We’ve reduced the amount of coag studies we’re getting on our routine trauma patients, probably about time we make sure we’re doing the same in our low-risk chest pain patients.
Can they eat?
Thoughts from Dr Ruben Strayer (who provided a great deal of our PSA card information) on enforcing fasting in the ED prior to sedation. No benefit, maybe even some harm? Don’t tell the folks at Kosair.
The Big Fat Suprise
Cool new book arguing it is ok to eat bacon, eggs and butter. My copy is due to arrive in the mail today.
Even cooler are these old articles (below) about CAD and MI that another author posted on his website in a review of the Fat book. Check out the articles. And this one written a few years ago. You’ll be drinking guiltless Breve lattes in no time.
Best App since Spotify
Just like Spotify, the QX Read app seems too good to be true. And free. I’d pay $5 or $10 for this little guy. Thanks to Cunningham for letting me know about this one. There could be other similar apps but this one so far has no shortcomings.
The app lets you perform literature searches, follow journals, follow keywords, follow collections you or other users make. It checks for new articles using your keywords and specialty interests. Best feature is you can login with the UL Library Proxy and while you read the abstract of the article, the app is getting permission for the article and you can open the pdf in seconds. Then open the app in your cloud app to save.
I’m sure you all get as frustrated as I do trying to use your phones to search for and download articles through UL’s library website ; ).
Ultrasound lectures
These are some great ultrasound lectures w/ videos from the EM program at MUSC.
Ketamine’s Kryptonite
I witnessed the third patient to have apnea as a side effect of ketamine administration. As in the other two cases ketamine was infused as a push, rather than the slow administration. This was not the resident, but typically and to be by the book, MDs should be the ones pushing ketamine. SLOWLY.
In this case our resident did well managing the sedation. Hypoventilation was diagnosed well before desaturation. Painful stimuli did not induce respirations as the ketamine is too good of an analgesic. We began to BVM ventilate, placed nasal trumpet, sat was never lower than 85%. Took about 8 minutes to get spontaneous respirations. We gave narcan as the patient had fentanyl prior to ketamine. As in one other case of ketamine apnea the narcan did not help, but should be attempted.
So learning point. NEVER SLAM ketamine into the patient. Dilute the 1cc (50mg-100mg) of ketamine in 10cc of saline if it will help the temptation to push it.
Also follow the algorithm below for PSA intervention. We will have the sedation review sheet and reference card finished soon.
Public health for adrenaline junkies
Public health is associated with the least interesting courses of medical school (epidemiology and biostatistics). It has been linked to ED frequent flyers and psych hold patients (social and behavioral health). One might say it’s an integral part of vague clinical decision rules and flip-flopping society guidelines and Press-Ganey scores.
It’s also something us ED docs do every day, whether we want to or not. There’s no reason why we shouldn’t try to understand it and do it better.
Kiran and I have been developing a website dedicated to public health for ED personnel. It’s a FOAMed site. Our plan is to get it tied in with sites like EMCrit, ALiEM, LITFL, and the like. It’s still a very young project, but there’s a couple articles posted for you to glance at.
If anyone is interested in population health, there’s a ton of uncharted territory and we’d welcome the collaboration. Just let us know how you want to be involved. Also, tell your friends.
Special
Here is a very practical algorithm. I recommend using it every shift.

Source: life in the fast lane?
Burnout
Brief description of burnout types. Not medically specific. Follow the links as well.
1. Overload: The frenetic employee who works toward success until exhaustion, is most closely related to emotional venting. These individuals might try to cope with their stress by complaining about the organizational hierarchy at work, feeling as though it imposes limits on their goals and ambitions. That coping strategy, unsurprisingly, seems to lead to a stress overload and a tendency to throw in the towel.
2. Lack of Development: Most closely associated with an avoidance coping strategy. These under-challenged workers tend to manage stress by distancing themselves from work, a strategy that leads to depersonalization and cynicism — a harbinger for burning out and packing up shop.
3. Neglect: Seems to stem from a coping strategy based on giving up in the face of stress. Even though these individuals want to achieve a certain goal, they lack the motivation to plow through barriers to get to it.
In a roundup of 11 ways to beat burnout, 99u offers this breakdown of the three main types of burnout, per the Association for Psychological Science.
Pair with this essential read on how to transcend the “OK plateau” of work, then see how sleep factors into the equation.
Here is the article itself from APS.
Reference:
http://explore.noodle.org/post/83726976259/1-overload-the-frenetic-employee-who-works?utm_content=bufferef345&utm_medium=social&utm_source=twitter.com&utm_campaign=buffer
The Hypercoagulable Liver Failure Patient?
Hey Guys,
Just listened to a portion of April EM:RAP (so if you’ve heard it already here’s a little repetition) and was surprised to hear their Notes from the Community Section about coagulopathy in Liver Disease, which basically informed me that many liver patients are at just a high of risk of thrombosis as they are of bleeding.
3 Articles were referenced:
– Tripodi A, Mannucci PM. The coagulopathy of chronic
liver disease. N Engl J Med. 2011 Jul 14;365(2):147-56.
– Villanueva C et al. Transfusion strategies for acute upper gastrointestinal bleeding. N Engl J Med. 2013 Jan 3;368(1):11-21.
– DeLoughery TG et al. Invasive line placement in critically ill patients: do hemostatic defects matter? Transfusion. 1996 Sep;36(9):827-31.
Summary:
– The liver makes both procoagulant and anti-coagulant proteins which can be actually reduced close to equally rendering the patient basically in equilibrium (thus not so hypercoagulable).
– No study has shown that coagulation defects predict issues with procedures (but the experience of the clinician performing the procedure does).
– INR is not standardized in Liver Failure patients (like it is with Warfarin) and thus is not that helpful.
– PT & PTT may also not be helpful in patients with liver failure (due to the variability of loss of clotting factors)
**Fibrinogen may be low in liver failure patients, and you may consider replacement of this with Cryoprecipitate (10 units of Cryo increases the Fibrinogen by 100mg/dl).
– Raising intravascular volume with pRBCs may make them bleed more.
For the full references & discussion see the EM:RAP written summary. Perhaps this is something we should discuss with our GI colleagues and/or MICU people. Any thoughts?
Wellens’ Or Not?
A middle aged male presented for evaluation of AMS; he had agitation, confusion, and tremors. He has a history of Bipolar disease and schizophrenia as well as HTN. Vital signs were all stable on presentation and within normal limits. On exam he was oriented only to name, but not place or time. Neurological exam was normal, with the exception of tremors. Med list includes Haldol Injection, Lithium, Benztropine, Olanzapine, and Propranolol. At this point, I was not quite sure what is going on with him, so I had a bit of a shotgun approach. Initial EKG revealed the EKG below.
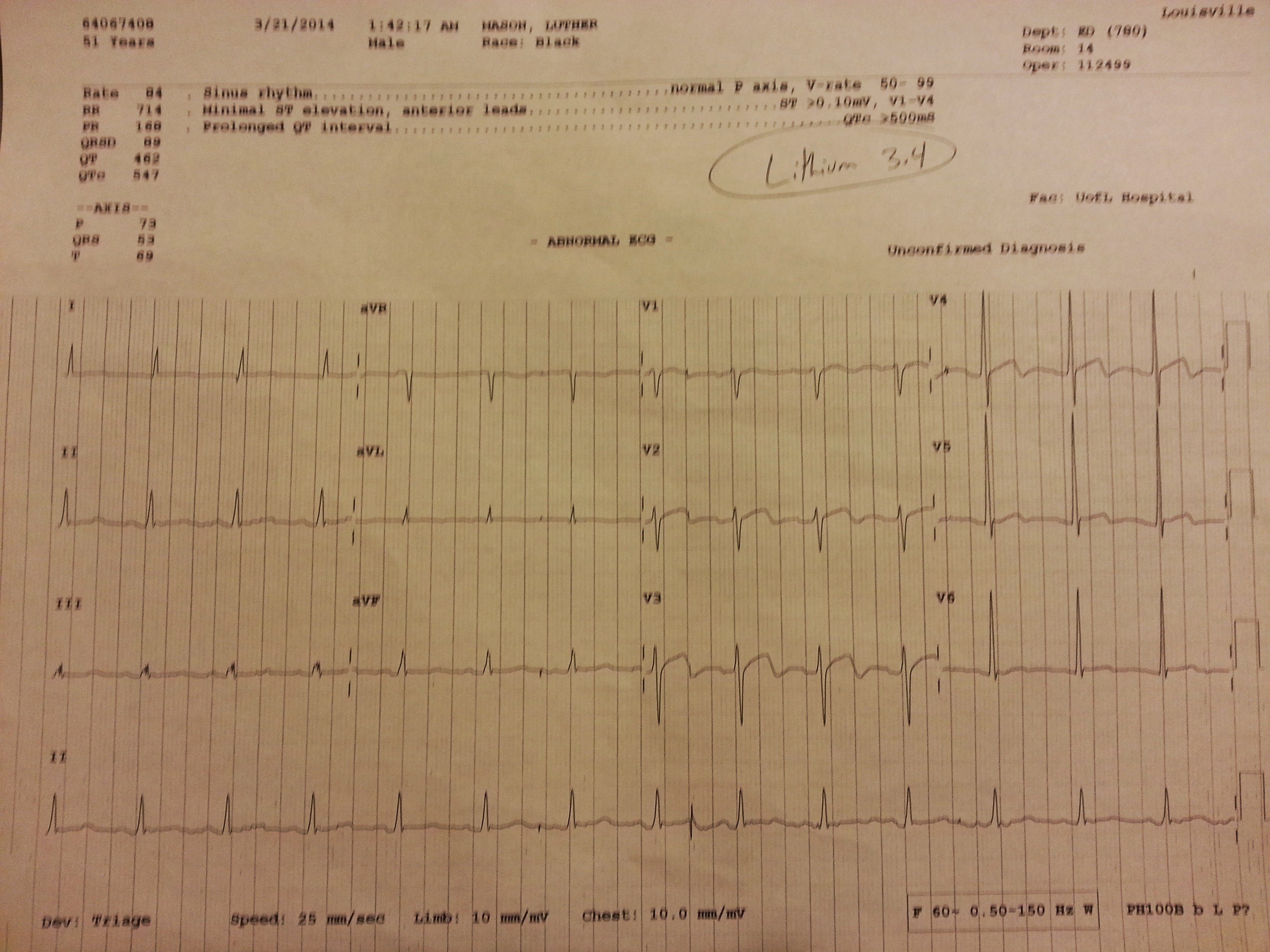
It appears to be similar to Wellens’ syndrome but not consistent with my gentlemen’s symptoms.
A quick literature search revealed a case report showing lithium induced EKG changes, similar to his EKG above. Further supporting his lithium induced changes in this scenario is no clinical findings to suggest ACS, and a negative troponin 3x. He was ultimately admitted and treated for lithium toxicity, without any cardiac complications.
EKG changes seen in lithium toxicity:
– ST elevations (1 other single case report)
– QT prolongation
– non-specific ST segment changes/T-wave abnormalities
FOAMed and Social Media in Education
At the CORD Academic Assembly there was a lot of talk about FOAMed and Social Media. I am on the social media committee with CORD and we have some informative projects on the horizon.
Here is a blog post detailing some of the FOAMed workshop with some How-To information.
Then Joe Lex and Nicholas Genes posted PRO and CON articles on the question “Is FOAMed essential to Emergency Medicine education.”
Not long articles, good to be at the forefront of these changes. And good discussion on the pluses and minuses of FOAMed