![Room9er ["Room Niner"]:](https://room9er.com/wp-content/uploads/2020/03/cropped-Screen-Shot-2020-03-08-at-3.16.16-PM.png)
Here is the powerpoint, will post the tegrity file when available.
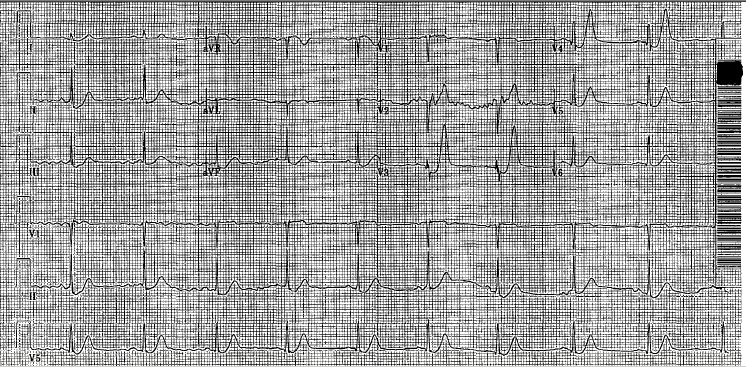
The elusive S1Q3T3
So this is a case I thought was interesting that I had in the department back in May. We all know that the most common EKG finding in the setting of PE is sinus tach, however the pimp question that is also asked is the finding of S1Q3T3. While I can easily recite the alphabetic-numeric code S1Q3T3 by heart at the drop of a hat, I had never seen one and honestly thought I never would. I thought finding S1Q3T3 was likely as rare as surviving a ED thoracotomy (OK maybe not that rare). So on to the case.
39 year old female presents to the ED complaining of SOA and cough for the past two weeks. Cough was productive of green sputum, no fevers, and she does complain of some chest pain which sounds pleuritic in nature. Initial vitals HR 118 BP 111/73 RR 16 O2 97% room air. As I get into her PMH she says she has a history of multiple PEs with an IVC filter placed 1 yr ago because apparently she wasn’t very good at remembering to take her coumadin. She has had a hypercoagulability workup which was negative, no recent travel, no estrogen use.
So at this point with a history of multiple PEs, tachycardia, SOA, and pleuritic chest pain I am thinking I am going to scan this lady. Even though she had a IVC placed a year ago, she is still saying all the right things for PE. So while the CTPE protocol was cooking I got an EKG and there it was, S1Q3T3!

Needless to say I was pretty excited and immediately showed the rotating intern next to me who clearly didn’t share my enthusiasm. When I compared this new EKG to a past EKG a month ago she did not have the S1Q3T3.During her admission a month ago, when she had a normal EKG, she had a CTPE showing a chronic PE. This time when her CTPE came back the read was Acute on Chronic Pulmonary Embolism. So a month ago she had a chronic PE with a normal EKG and at this visit she had an EKG with S1Q3T3 and a acute on chronic PE. Out of curiosity I dug through her medical history a little bit more and found that this patient had multiple prior admissions for PE with multiple CTPE protocols and EKGs. What I found was that whenever this patient had a CT read of Chronic PE she had a normal sinus rhythm EKG. However, whenever she had a read of Acute on Chronic PE (which was 4 times!) she had a EKG showing S1Q3T3, dating all the way back to 2012. Yea, apparently this lady has been hanging out with a chronic PE in her distal right main pulmonary artery since 2012 and every once in a while she will throw a new small PE, even with an IVC filter.
So after doing a little bit of thinking and a little bit of reading it made sense. The EKG finding of S1Q3T3 is indicative of right heart strain, in this case resulting from an acute PE. So this patient’s heart has adapted to her chronic PE, however every time she throws a new PE she has an element of right heart strain which can be seen on her EKG as S1Q3T3.
I just thought this was pretty interesting to actually see the physiologic and mechanical adaption and strain this patient’s heart was undergoing being clearly demonstrated on her EKG. Also I learned that S1Q3T3 is not like a q wave after an MI in that it stays on the patient’s EKG, it is a finding that comes and goes depending on the patient’s presentation.
Anyways I thought this was a pretty cool little case and figured I would share. Hope you all enjoyed.
The Kitchen Sink
Fairly early into an overnight shift the radio goes off. EMS is approximately 6min out with mid 30s male undergoing CPR. Per bystanders, the patient was going running from door to door, banging on doors and yelling for help. Shortly after being taken into police custody he was found to be pulseless. Had been undergoing CPR approx 10 min. King airway in place. No improvement with dextrose and naloxone.
The intern on and myself go to Room 9 to get set up. When EMS arrives about 10 minutes later, CPR is still ongoing and rhythm has been asytole/PEA throughout. The story remains consistent with him going from door to door yelling for help but now there is some variation as to whether he was cuffed and then lost his pulse, was found without a pulse, or if he got into a physical altercation with the neighbor and then lost pulse shortly after arrest. There are no signs of trauma and we elected to not invite additional chaos by calling a Level 1.
CPR is continued. King airway switched out for ETT. Accucheck 250’s. Central venous access and bilateral chest tubes placed with no rush of air or blood. Sats persist at 85% on vent, etco2 is in 60’s. He gets epi q3m. A dose of vasopressin and steroids. Istat has K 5.5. Lactate >20. Received 2-3 amps of bicarb. Received calcium. Upon rhythm checks he was primarily asystole except for 2-3 checks with a narrow pea that would not persist. Each time the ultrasound was placed on his heart there was no cardiac activity. My thought process at this time was that he was either excited delirium that I’m not going to be able to do much about or some kind of ingestion/overdose. We called pharmacy and asked for lipid emulsion. His ETCO2 had remained between 40-60 and we were about 40 minutes out from reported time of arrest. I decided if the lipids were unsuccessful that would be when we would call it.
They arrived about 15 minutes later and were infused. By now his etco2 had drifted down to 10 on the most recent pulse check. No changes occurred and TOD was called.
Reasons not to get into prison fights…
Middle aged male transferred from an OSH, accepted by ENT for a mandible fracture.
The patient is incarcerated, and was involved in an “altercation” with other inmates. The incident occurred around 2PM; but he didn’t report any of his pain to the guards until 10PM. On arrival at the OSH he had multiple contusions to his face/head, lacerations over his hands, and obvious dental trauma. The patient was also complaining of chest pain – he stated that another inmate had slammed him in the chest with his knee. Despite his age, the patient has a history of previous MI in 2011, cathed at U of L with no stents placed. Takes a baby aspirin, no other meds and no other PMH.
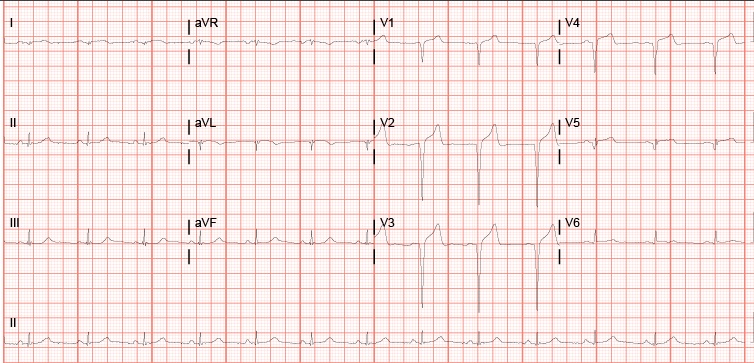
At this point, the patient is about 10 hours out from the incident. Work-up at the OSH with the following: neg CT head and CXR. CT face with a mandible fracture. Labs notable for WBC 17.8, Hgb 14.3, platelet 373, normal coags, normal electrolytes, BUN/Cr 14.0/1.1. Total CK 213 (55-170 normal), troponin <0.012, CKMB 1.66 (0 – 3.38 normal), myoglobin 271.8 (0-121 normal). Tox screen negative. EKG is as follows:
His hand lacerations were repaired and he was started on Augmentin for a human bite. ENT accepted, and the patient was transferred to U of L, arriving about 6 AM. Dental was consulted on arrival and splinted his teeth. By 9 AM ENT had evaluated the patient and admitted him to the floor, planning for surgical intervention.
The patient was an ED floor hold, and around 2PM began complaining of worsening chest pain. ENT was paged and ordered an EKG and a set of cardiac enzymes, coming down to re-eval the patient. His EKG now looked like this:

Enzymes came back with CK total 5024, CKMB 303, and troponin 44.1. Cardiology was consulted and ordered a stat echo and started the patient on ACS protocol. The echo showed an EF of 30%, an akinetic mid/distal anferoseptum and an akinetic apex. Cards initially thought that this was consistent with stress cardiomyopathy in the setting of trauma, but couldn’t rule out cardiac ischemia due to direct cardiac trauma. They planned to treat medically and cath in the morning.
Throughout the evening, he developed worsening ST elevation in his lateral leads and his troponin continued to rise, up to 67.0 by midnight.
The on call cath attending at Jewish was consulted and by about 3AM the decision was made to transfer the patient to Jewish for a cath first thing in the morning.
Final result: 100% LAD occlusion, secondary to direct cardiac trauma.
Definitely rare injury, but one to keep in the back of your mind, especially as it can occur in previously healthy, relatively young patients. Of note, these can have delayed presentations, up to several days. Typically occur after MVA, but there are several cases reports occurring after crush injuries, being hit in the chest by a soccer/rugby ball, and my personal favorite, one listed as “struck in the chest by an umbrella tip.”
My brain hurts
Hey this is not a case but what goes through my own head on a difficult shift. There is a lot of information out there on cognitive load / error. Dr Croskerry is essentially the EM world expert on this subject. Take a look at this most recent article. Another great resource are a couple books, one short and sweet the other very in depth. Both are dirt cheap now on Amazon.
Pacemaker identification from CXR
This is a neat party trick I picked up on CCU. Now when a patient comes in with pacemaker malfunction/chest pain/syncope and needs a Cardiology workup and admission, but hasn’t been able to locate their pacemaker card since the mid 90’s, you can look like a pro and know the device manufacturer from CXR alone (which is something we get anyway on anyone who remotely looks like they might need Cardiology).
Paper and algorithm can be found here:
http://www.ianchristoph.com/physician-resources-2/device_id.pd
Ready for discharge?
Interesting case from my MICU month. Pt is a middle aged WM with hx of HIV, CVA presented to the ED with hypoxic respiratory failure and sepsis. Intubated in the ED and admitted to the unit. Pt self extubated few hours later in the MICU. Responded well to fluids, antibiotics and O2 nasal cannula. Few days later, nurse d/c’ed his RIJ central line.
Within minutes, pt became severely altered, O2 sats plummeted to the 60s and bedside ultrasound showed significant air bubbles in the cardiac chambers.
What happened? When central line was removed, the wound site was not immediately occluded (with fingers, dressing with tape, etc). As pt inhaled, air traveled through the communicating conduit into the central blood vessel.
What to do now? Intubate for severe respiratory distress. Place pt in left lateral decubitus position and Trendelenburg position–prevents air from traveling to the pulmonary arteries causing airflow obstruction. Hyperbaric oxygen therapy, if you suspect cerebral embolism, as it decreases mortality.
The pt was intubated, placed on his side with bed tilted down. Did fine and transferred to floor the next day.
Meat Sweats
I know I have had the postprandial coma, not sure about the meat sweats. I love the “localizes to bacon.” Not trying to be insensitive to anyone with weight problems, we have all been low on this GFCScale!
Positioning is Everything
When using a chest x-ray to look for a pneumothorax, positioning of the patient is everything. The first chest x-ray below is an upright chest x-ray from an OSH of a patient that fell 30 feet from deer stand and was found to have a right pneumothorax. The OSH didn’t do any other imaging and didn’t even send the patient with a c-collar.
When the patient arrived we laid him down and placed a c-collar and assumed that his spines weren’t cleared yet. When we shot the portable, supine chest x-ray in our ED we couldn’t see a pneumothorax and our radiologist actually read it as no pneumothorax.
Using the US, an EFAST was performed and showed a pneumothorax and the subsequent Chest CT verified it. Therefore the next time you get an ED, supine chest xray on someone, remember that just because you don’t see a pneumothorax on a supine CXR, doesn’t mean they don’t have one. The optimal xray is an upright chest xray (expiratory if possible)!
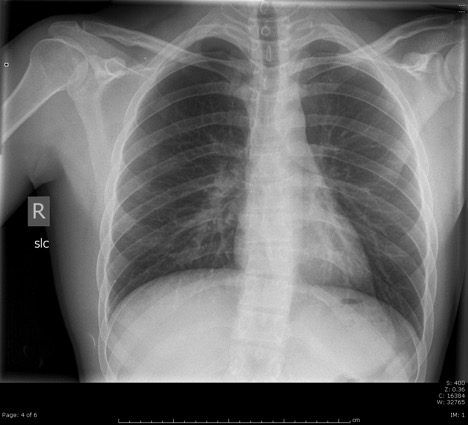 Upright Chest x-ray from OSH
Upright Chest x-ray from OSH
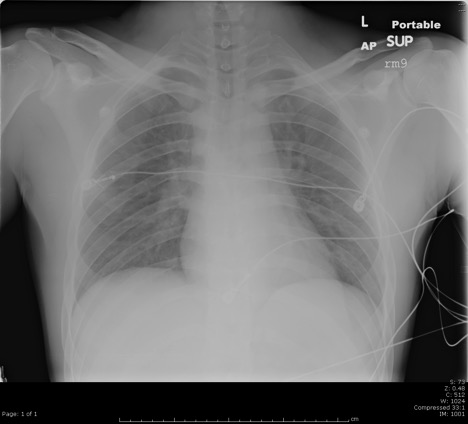
Portable, supine Chest X-ray in our ED
CT showing the Right Pneumothorax
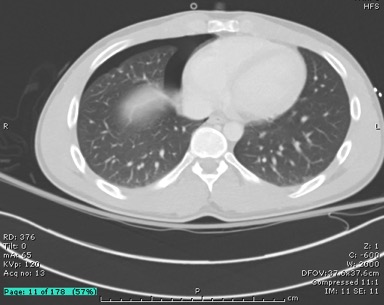
Acute Cholecystitis, Classic
Interesting case from a couple weeks ago.
20ish yo white male, no significant past medical diagnoses. Overweight. Family history of gallbladder disease. No OTC or Rx medications. Patient smokes, does not drink, and has used IV drugs in the past.
Here in the ER due to RUQ abdominal pain for one week, was coming and going and is now constant. On further questioning, admits that his mom made him come because of her history of gallstones and cholecystectomy. On exam patient has jaundiced sclera and urine on table is dark brown, pain in right upper quadrant of abdomen is exquisite. States he has been vomiting especially after eating and all food makes him sick. No documented fevers, but feeling chills.
Urine: Large bilirubin, otherwise normal
Pertinent blood: WBC 8.4, Hgb 14.2, Plt 430. Alk Phos 140, AST 734, ALT 1417, Total Bili 9.5. Lipase 22. Tylenol neg.
Didn’t expect this guys ‘acute chole’ to cause liver failure. Either way, he was getting further imaging to find out more. No ultrasound coverage at 5am so CT for now, then ultrasound at 7am. Added tox screens and hepatitis panel at this time.
CT abdomen/pelvis with contrast: “Markedly thickened/edematous wall of the gallbladder indicating cholecystitis. No calcified stone visualized. Additional imaging maybe obtained with ultrasound.” Also, normal liver.
The results of the ultrasound showed a “nondistended gallbladder with marked wall thickening, edema and a positive sonographic Murphy sign. Given lack of clear visualization of the posterior wall, highly worrisome for complicated cholecystitis, possibly gangrenous or with a focal posterior perforation.” Normal liver and mildly dilated bile duct.
Now with labs showing liver failure and two forms of imaging showing acute cholecystitis, it had to be. Admitted to the general surgery team though the ‘acalculous cholecystitis’ with liver failure was enough to peak my interest in follow-up.
Hepatitis panel comes back later same day showing reactivity for Hep C. Discharge 5 days later, no surgery, no acute interventions, with down-trending liver function panel and follow-up with the GI clinic.
While most commonly associated with cholecystitis, a quick literature search reveals multiple reasons besides cholecystitis to have gallbladder wall thickening… congestive heart failure (right sided), gallbladder carcinoma, adenomyomatosis (chronic gallbladder inflammation or degeneration), renal failure, pancreatitis, cirrhosis and other forms of liver failure.
Just some thoughts on stroke management in the acute setting…
A couple months ago (during lecture), we had a discussion regarding tPA and acute onset of stroke. As you would expect, we discussed the indications, contraindications, etc of treating stroke with tPA. We also touched on the subject of our role in pushing tPA here at UofL.
Obviously as a stroke center, our stroke team is working around the clock- and as such, generally takes the ball on this one. However, when we are practicing outside of UofL, a stroke team is not always going to be available and ultimately the management will fall on us. Hence the discussion and considerations for us making the call or at least working towards that possibility in the future.
Coincidentally, at precisely the same time as this conversation, a small journal, based out of New England, with a primary focus on medicine, published three fine articles on a similar topic. These articles were focused on the treatment of stroke in the acute setting.
As pertinent to this post, they explored the use of thrombolysis as well as mechanical removal of thrombus when said thrombus is located in a proximal vessel. Now I won’t pretend I can read, but for those of you who can- below, are links to two “previews” and one complete view of the above mentioned articles. Additionally, an audio file is embedded, containing a break down of the articles by Dr. Dave Newman, of the Mt. Sinai School of Medicine in the Department of Emergency Medicine, to be featured on a future episode of EM:Rap.
Ultimately, I guess the questions I have regarding this as a post on Room9er are as follows:
1. I believe the Stroke team has embraced these articles and to my knowledge (as of February) may have moved towards mechanical retrieval of thrombus in proximal vessels in appropriate candidates. If we are trying to move towards a more ED involved decision tree, what will we need to know and where will our policies stem from? At least as a concept. At this time, I have only heard us discuss tPA, but if we as a hospital are moving towards multiple modalities for treatment of acute stroke, should we not be discussing these as well?
2. With consideration of a 6 hour time frame to thrombus retrieval, what is our (UofL) policy on timelines regarding retrieval. (This is not reflecting any current policies, merely one parameter from one study.)
3. How much time is required from page to cath? This is undoubtedly a big question. What does it take to have a vascular team, NES team, etc ready do go. How will this influence our time of onset to treatment guidelines.
4. Outside of UofL, taking into consideration transit time, etc. how will this influence the management of stroke? Based on CTA availability, transit time, local resources, etc.
Cardiology
If you’re like me, and I know you are, you wish Martin Espinoza’s lectures were recorded and available. They are. You’re welcome.
Also, if you haven’t heard yet, the IM department just launched a FOAMed website called Louisville Lectures. It’s one of the first of its kind worldwide and it’s based out of ULH. Michael Burk, who is rotating with us this month from IM, is the founder and managing director. It got a shout-out on LITFL this month. Worth a look.
Changes to tPA Contraindications in Acute Ischemic Stroke
Since its approval in 1987, controversy has surrounded a drug that we all know is near and dear to my heart, recombinant tissue Plasminogen Activator (insert eye roll). In similar discreetness of a Hollywood wedding, the FDA updated the prescribing information of tPA with important changes made to the contraindications to the use of tPA in the setting of acute ischemic stroke. It is unclear as to what prompted these updates and why. There have been no recent studies of significance published to support these modifications.
2/2015 updated prescribing info:
“Do not administer Activase to treat acute ischemic stroke in the following situations in which the risk of bleeding is greater than the potential benefit:
• Current intracranial hemorrhage
• Subarachnoid hemorrhage
• Active internal bleeding
• Recent (within 3 months) intracranial or intraspinal surgery or serious head trauma
• Presence of intracranial conditions that may increase the risk of bleeding (e.g., some neoplasms, arteriovenous malformations, or aneurysms)
• Bleeding diathesis
• Current severe uncontrolled hypertension”
Now contrast the new package insert to the 2013 package insert. Pay special attention to the omissions of the exclusion of contraindications in patients with history of intracranial hemorrhage and seizure at onset of stroke. It is pertinent to note that the wording regarding the contraindications has also changed. The previous consequences being “significant disability or death” have now been replaced with “situations in which the risk of bleeding is greater than the potential benefit.”
From the 2013 package insert (changes are italicized):
“Activase therapy in patients with acute ischemic stroke is contraindicated in the following situations because of an increased risk of bleeding, which could result in significant disability or death:
- Evidence of intracranial hemorrhage on pretreatment evaluation
- Suspicion of subarachnoid hemorrhage on pretreatment evaluation
- Recent (within 3 months) intracranial or intraspinal surgery, serious head trauma, or previous stroke
- History of intracranial hemorrhage
- Uncontrolled hypertension at time of treatment (e.g., > 185 mm Hg systolic or > 110 mm Hg diastolic)
- Seizure at the onset of stroke
- Active internal bleeding
- Intracranial neoplasm, arteriovenous malformation, or aneurysm
- Known bleeding diathesis including but not limited to:
o Current use of oral anticoagulants (e.g., warfarin sodium) or an International Normalized Ratio (INR) > 1.7 or a prothrombin time (PT) > 15 seconds
o Administration of heparin within 48 hours preceding the onset of stroke and have an elevated activated partial thromboplastin time (aPTT) at presentation.
o Platelet count < 100,000/mm3”
The new 2/2015 update does provide some vague conditions in which the risks of bleeding must be outweighed against the anticipated benefits (however, note that these are not firm contraindications):
• Recent major surgery or procedure, (e.g., coronary artery bypass graft, obstetrical delivery, organ biopsy, previous puncture of noncompressible vessels)
• Cerebrovascular disease
• Recent intracranial hemorrhage
• Recent gastrointestinal or genitourinary bleeding
• Recent trauma
• Hypertension: systolic BP above 175 mm Hg or diastolic BP above 110 mm Hg
• High likelihood of left heart thrombus, e.g., mitral stenosis with atrial fibrillation
• Acute pericarditis
• Subacute bacterial endocarditis
• Hemostatic defects including those secondary to severe hepatic or renal disease
• Significant hepatic dysfunction
• Pregnancy
• Diabetic hemorrhagic retinopathy, or other hemorrhagic ophthalmic conditions
• Septic thrombophlebitis or occluded AV cannula at seriously infected site
• Advanced age [see Use in Specific Populations (8.5)]
• Patients currently receiving anticoagulants (e.g., warfarin sodium)
• Any other condition in which bleeding constitutes a significant hazard or would be particularly difficult to manage because of its location.
Currently the guidelines have not updated their list of contraindications to tPA in acute stroke, but I wouldn’t be surprised to see them included when the guidelines are updated.
So like Oprah says, you get tPA! You get tPA! Everyone gets tPA!
Sinus tach Part II
This is a case that ended up being a 72 hour return. Another good example that sinus tach should have a good explanation. Another good reason to know discharge vitals!
Middle aged M, history of TBI, PE, MRSA bacteremia, s/p trach/g-tube/IVC filter, presents with displaced g-tube and increased agitation. Trauma consulted, g-tube replaced. Fluro shows good placement. Exam otherwise unremarkable. No labs performed. Documentation of to be non-verbal/not following commands and this was baseline. VS prior to discharge. Normal BP, HR trend: 68->70->115->111 (at discharge)
Patient returns for changed mental status. Not documented in what way he was changed from baseline. But found to have BUN: 115., Cr: 2.96. BP 90’s systolic, HR wnl. Head CT negative. Hgb: 12, INR: 1.6 (on coumadin) Na: 154, Cl: 112. Otherwise labwork unremarkable.
Patient admitted to medicine service. Hgb trended down 12.4->9.8->8.4. Patient receiving IV fluids during this time. Mild improvements in BUN/Cr. Patient was a STAT response 5 days later. Hypotensive/tachy. Hgb: 5.3 Dark stools noted. Transferred to MICU. GI scoped, found to have erosion of IVC filter into duodenum. Vascular consulted. Patient transfused/stabilized. IVC filter removed, transferred to floor. BUN/Cr normalized during stay.
Two things here, the HR as mentioned, should always have a good explanation. In a patient like this, the history is limited, more information is probably useful than less. Granted a patient like this is very difficult to evaluate at baseline, I’d lean towards shotgun labs/imaging etc. Not sure if it would’ve made a difference in the end but nonetheless.
On the 2nd visit though, a BUN of 115 should raise an eyebrow That’s a BUN/Cr ratio greater than 20. This patient could be just a simple AKI due to hypovolumia. But a BUN that high should also raise the suspicion of a GI bleed. A hemoccult probably is indicated at this point (for somebody that can’t relay much information at baseline). I don’t think anybody would’ve predicted the cause, but nonetheless, neither any of us, nor IM really interpreted that BUN as it should’ve. Just a few notes on Bun/Cr below taken from life in the fast lane. Not definitive, but just something to do a double take on.
Urea:Creatinine Ratio (in the setting of renal failure / elevated creatinine)
20:1 – normal or post renal cause of AKI
>20:1 – pre-renal cause (urea absorption increased compared to creatinine)
<20:1 – intrinsic renal damage (urea unable to be absorbed -> become like creatinine -> ratio gets closer to 1)
Ophtho
Hey folks,
Just wanted to share a little treasure I found a few years ago and may be of some use to others. This website is awesome for eyeballs, there is all sorts of instructional videos and pathology-related videos. The link below is about the basic slit-lamp exam. It includes how to use the scope, how to do the exam, what to look for, and some basic examples of pathology. The full website is at rootatlas.com , but if you’re a beginner with eyeballs (as I fear I may always be), then I’d start with this guy:
http://www.rootatlas.com/wordpress/video/874/slit-lamp-exam-video/
To FOAM!
–Zach