One of the most interesting posts recently was Zach’s post about what he could have done differently. Thought I would continue this trend and post a couple of cases that could have gone better and leave some things up for discussion. Case one here and two next post.
Case #1: 90 yo F h/o HTN and arthritis, restrained passenger of moderate speed MVA, driver was unharmed but car was going too fast and struck the back of a semi-truck. Extrication about 10 minutes. Patient c/o right leg pain and right forearm pain, skin tear to right arm and obvious Colles fracture and femur fracture likely as well on initial exam. No chest or abdominal pain. Kept in R9 for the potential femur fracture and age. Vital signs all been stable, patient a&ox3, talkative and despite mild pain appears in good spirits.
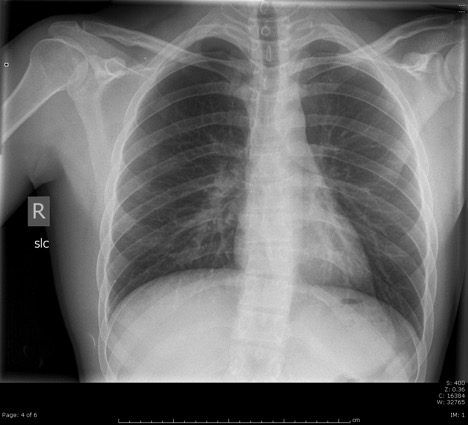
On initial exam, HR 96 and regular, 125/70, RR and temp normal. Pain controlled as long as not moving. Good breath sounds, minimal chest tenderness on palpation of sternum, abdomen and pelvis unremarkable. Placed in traction splint in R9 for significant pain and shortening of right leg. CXR normal, PXR normal, and R femur with proximal femur fx minimally displaced. FAST neg. Give tdap and bag of LR. Further eval shows pain in right leg from femur/knee/tib/ankle and also left femur/knee/tib. As mentioned obvious fx right Colles, with pain in right elbow/forearm/wrist/hand and also pain left forearm and wrist. That makes for man scan + a whole ton of xrays in all extremities.
Spoke with ortho on the phone in R9 due to known femur fracture. Vitals on R9 exit unchanged. To the CT scanner. Nurse calls from xray after CT done and asks for small amount pain meds as patient now c/o more pain, especially in right leg and arm. Dilaudid 0.5mg ordered. Patient comes into main ER literally 90 minutes after initial presentation due to so many xrays! (This is my fault). Labs unremarkable, Hgb 11. I see the CT scans but nothing obvious to me, no head bleed, no c-spine fx, no PTX, no obvious free fluid in belly. See patient as she as she comes back bc ask for more pain meds. HR now 120s, irregular?, BP 95/65. Ask nurse how long this has been going on, states “oh, just the last 30 min or so.” Ortho at bedside as well, wants to do sedation.
EKG done, show afib rate 120s (no h/o afib). BP cont to be 90/60s. Giving 2nd L LR, nurse start 2nd IV and get L NS going. Patient still talking and states she feels ok other than the pain in her leg. Call to Trauma (should have called earlier in 90 yo with known femur fx), but by now its been more than 100 min total time in ER. Trauma arrives pretty quickly, patient now been here 2 hrs. Agree with fluid boluses, talk about patient condition with fellow and wedge and all agree think likely due to trauma in afib and that why BP sucks.
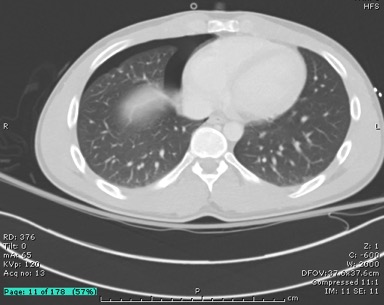
Tell ortho that too high risk patient and unstable to do sedation. Does hematoma block right Colles fracture with reduction as well and leaves the femur in traction. Admitted to SICU after just over 2 hours in ER. CT head and c-spine only scans back and are neg at admission. About 30 min later rest of man scan comes back. Small nondisplaced sternal fx and very small hematoma (but possibly active bleeding) to right retroperitoneal area. Again speak to trauma about this. Asked about the retroperitoneal bleed and fellow states it very small and should wall off without intervention based on place. Possibly afib due to contusion? Cards was consulted by Trauma who saw patient and said to control pain, resuscitation and other trauma factors (unhelpful but true, not much for them to do).
Brings up a question I had, in setting of trauma, what medicines should be given for afib with RVR? Cardiac contusion? Or just let it ride? Trauma asked the nurse to give metoprolol but this was never given mainly due to nursing concerns about BP.
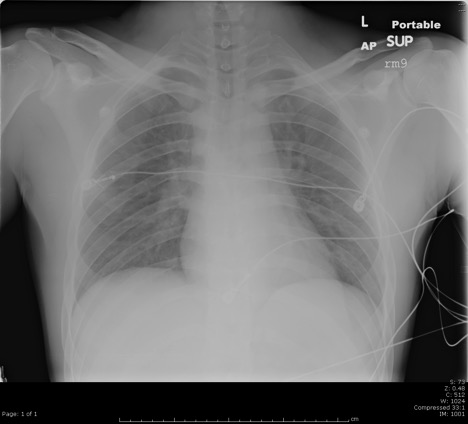
Ok, long story short, HR cont to be 120-130s, afib, BP 90/60s, after being ICU hold for about 2 hours patient had decreasing mentation. Trauma placed central line and a-line and ABG showed pH 6.8! Istat Hgb 8.0. Blood given, minimal response.
Patient intubated by trauma, arrested during intubation, one round CPR and came back, went to SICU same vitals, called in IR and intervention showed minimal bleeding, thought to likely be venous, but did have several coils placed. More blood and then pressors through the night. Arrested 2 more times throughout the next 6 hrs, family still wanted all interventions. Finally about 12 total hrs after ER presentation, arrested for about 20 min and TOD called.
Couple of main points from this case that I learned and hopefully helpful for you all:
1. As Coleman says, old people go down hill quickly, be on your guard no matter how good they may look on presentation.
2. Be careful of ordering too many xrays, me not seeing the patient for over an hour while in xray is unacceptable, I should have known the change in her vitals either by seeing it directly or have nursing tell me.
3. I knew this was a trauma admit as soon as she hit the door being 90 yo and femur fx, but I didn’t call them for a long time, why? Bc I didn’t have much to tell them (couple xrays, stable VS, man scan taking 3 hrs to get read). But just be sure to get them involved early.
4. We don’t typically repeat labs or get istat too often, but for someone like this who takes a turn for the worse, would have been worth it to get hgb after her vitals became unstable.
5. Her mentation decreased after admission, but I could have been more aggressive with central line and resuscitation (blood), she got 4L crystal but needed products.
6. This one was pretty clear cut that should not do sedation, but don’t be afraid to tell ortho ‘no’ if you’re worried about their safety.
7. I’m sure there is more, would appreciate your thoughts and comments…
![Room9er ["Room Niner"]:](https://room9er.com/wp-content/uploads/2020/03/cropped-Screen-Shot-2020-03-08-at-3.16.16-PM.png)