Wellness Day
- Wellness rotation and fellowship – Reach out to Dr Huecker and Dr Dennison if any questions
![Room9er ["Room Niner"]:](https://room9er.com/wp-content/uploads/2020/03/cropped-Screen-Shot-2020-03-08-at-3.16.16-PM.png)
Wellness Day
Lightning Lecture – Tuberculosis by Hannah Hudson-Knapp
Lightning Lecture – Tetanus by Jonathan Mattingly
Teaching Strategies – Feedback Models by Matt Lyons
Question Review – Metabolic, Nutrition, Endocrine by Nicole Harris
R2 Pathway – Sepsis by Makayla Campbell and Olivia Stanforth
Image Review – by Dr Kahra Nix, Dr Jeff Baker, Dr Alex Bequer
McGowan – Teaching series
Scaffolding –
Ex )
Final thoughts
Coffman – Question
Kelesis – RM9 Follow Up
27 F w ho asthma, prior suicide attempt presents after unknown but large ingestion ibuprofen
VBG 7.3/33.5/82/-9.5
CHEM8 139/3.6/108/143/1.14
Lactic 5.0
Intubated for aspiration risk w prop fent
CXR ok
CT head ok
C/f for lactic acidosis (AGMA), bleed, kidney injury
Rpt gas w ph 7.1, lactic to 8.3, Gap 19
HD placed, admitted to MICU underwent HD, still admitted to 3N
Reversible binding COX1/2 -> depletion of thromboxane = bleed
Peak plasma concentration 1-2hrs
Activated charcoal within 2 hrs of ingestion can be considered
Davenport – Shock US
I – indications
A – acquisition
I – interpretation
M – MDM
Pump – heart squeeze, beating, effusion
Pipe – IVC – plump, collapsable
Problem
Cardiogenic shock
Obstructive
Hypovolemic
Distributive
VEXUS (on icu pts s/p open heart sx)
IVC widest diameter in subcostal view, >2cm moveone, less thant 2 = noncongestion
Hepatic vein w indicator towards pt head, find vein entering IVC
Portal vein w indicator towards back
Renal vein
Compare waveforms and grade
Obrien – Pituitary
Sheehan – pituitary grows in pregnancy but not blood supply, vulnerable to hypotension
Pituitary apoplexy
Acromegaly – excess GH from pituitary adenoma
SIADH –
Congenital hypopituitary
Optic chiasma – pituitary masses compress this
Prolactinoma – most common pituitary tumor
Zach; Vitamins
B1 Thiamine
B2 Riboflavin
B3 Niacin
B5 Pantothenic Acid
B6 Pyridoxine
B7 Biotin
B9 Folate
B12 Cobalamin
C
Caroline; Hypoglycemia
Lyvers; pediatric endocrine
Hypoglycemia
– Obtain critical sample during hypoglycemic <50 episode
– for metabolic disorders
Fatty oxidation
Insulin mediated
Ketotic hypoglycemia
Disorders of gluconeogenesis
Tx – Rule of 50
Hyperglycemia
Shaw; Acid Base
Look at pH (primary disorder) > check for compensation
Respiratory
Metabolic
Metabolic acidosis is usually complicated by compensation
Winters = paCO2 = 1.5 (HCO3) + 8 +- 2
Anion gap = Na – Cl – HCO3
NAGMA = GI vs renal bicarb loss
MUDPILES
Excess anion gap
Use base deficit to predict resuscitation goals
VBG for people that don’t need exact pCO2, pulse ox accurate
ABG for people in shock
R acidosis – minute ventilation
R alkalosis – treat underlying cause
M alk – stop offending agent, consider CA inhibitor
M acidosis – treat underlying cause
Bicarb- need control or respirations to make sure co2 is blown off
Thomas; DKA/AKA
Gluconeogenesis/ glycogenolysis not as efficient glycolysis
Gluconeo breaks down fats and proteins
Glyco
T1DM no insulin production
T2DM insulin resistance
Insulin = store
Glucagon = burn
T1DM more likely to have DKA
AKA
Wide gap acidosis in chronic drinkers
Due to shift of carb metab due to malnutrition
Alcohol w no glucose
S/Sx
Labs
Does not need to be acidotic
Padget
Alcoholic ketoacidosis
Presents; n, v, dehydration, ams
Suspect in poor po + alcoholism
Alcohol increases NADH/NAD+ = higher ketones and lactic acidosis
Dx overlaps to some degree w starvation ketosis, DKA
Tx
If lactic >4 something else going on
Disposition; resolution in symptoms, acidosis = home
Rizzo; small group
Case 1 – HyperK
Case 2 – HypoK
Case 3 – HypoNa
Case 4 – HyperCa
Case 5 – HypoMg
Ross; Small group
Case 1 – thyroid storms
Hashimoto – low thyroid
Exogenous – dont need ptu, methimazole
Case 2 – HTN emergency (pheo)
Case 3 – Myxedema coma
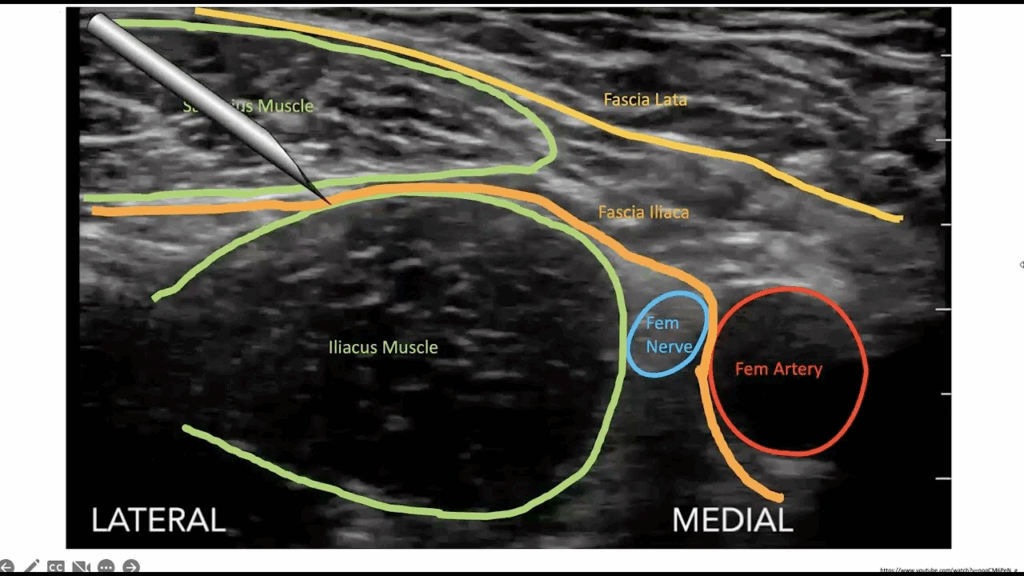
Bequer/Baker; US
Fascia Iliaca Block
Blocks femoral/obturator/lateral cutaneous nerves
Indications
Careful on anticoagulated pts
Ropivicaine/bupivicaine preferred (longer acting)
Use linear probe
2 person procedure
Enter laterally between fascial planes
Sickle Cell pain treatment
Pain triggers
Diagnositc criteria
Management points:
Pharmacy lecture
Myasthenic Crisis
Febrile seizure
Pharmacology
Stroke prehospital
TBI EMS
Central Venous thrombosis
Guillain- Barre
Acute dizziness
Functional Neurologic Disorder
Toxic Alcohols – Dr Eisestat
Ethylene glycol is a glycol and not an alcohol, however still included with methanol as the more toxic alcohols.
Isopropanol and ethanol can still be toxic but significantly less so than methanol and ethylene glycol.
Isopropanol
Methanol can be found in windshield washer fluid, solid cooking fuel, embalming fluid, and tainted beverages
Methanol
Ethylene Glycol
Can be treated with ethanol and fomepizole
Fomepizole
Anyone who has acidosis, clinical symptoms, or concentration greater than 20mg/dL gets treatment.
Hemodialysis
https://www.extrip-workgroup.org/ contains a list of recommendations for hemodialysis.
Pancreas – Dr Huecker
The pancreas is retroperitoneal and may not always show signs of peritonitis until very advanced disease.
Lipase will generally have to be 3x upper limit of normal to diagnose pancreatitis
Amylase sensitivity is less than 80%. Lipase is a better test.
CT
If CT is positive, the patient should be evaluated with ultrasound for concern of gallstone / biliary pathology.
Scorpions and autoimmune are rarer causes of pancreatitis
Management
Multiple scores such as BISAP and Marshall score can be used to risk-stratify
Most patients do not require antibiotics, however if there is extrahepatic infection or necrosis, it is necessary.
Imipenem and meropenem are specific antibiotics which can penetrate the biliary system well.
Abdominal hypertension is a potential very serious risk
Encourage early enteral feeding in mild cases
Pseudoscysts:
Pancreatic Cancer:
Pediatric Lower GI Bleeds – Dr. Lyvers
Usually occur inferior to the ligament of Trietz
80-90/100,000 complaints of peds ED visits
Some cases of suspected GI bleeding are not blood
Red Brick Diaper Syndrome
Cefdinir – Often a cause of red-purple stools
Some cases are blood but patients are not sick
Melena Neonatorum – Swallowed maternal blood during delivery or breast feeding, is the most common reasonof melena in a neonate. Can use the Apt test looking for HbF.
Anal Fissures
Some cases are a result of very concerning pathology
Midgut Volvulus – Occurs within the first month with bilious emesis and abdominal distention. Hematochezia is a late finding. Diagnosed by abdominal x-ray or upper GI series.
Nectrotizing Enterocolitis – Most commonly presents in pre-term infants in the NICU, however 13% occur in term neonates. Usually occur with underlying predisposition with sepsis or CHD. X-ray will show pneumatosis intestinalis or ileus in the early stages.
Hirschsprung’s Disease – Failure of neural crest cells to migrate during intestinal development resulting in aganglionic segments of bowel. Typically diagnosed as a failure to pass meconium in first 48 hours.
Hirschsprung’s Associated Enterocolitis – Can be seen 3 weeks to years after surgical repair. Abdominal distension, fever, vomiting, lethargy, foul smelling and bloody stools which can lead to shock. Provide with broad spectrum abx + metronidazole, as well as good resuscitation.
Meckel’s Diverticulum – Painless rectal bleeding caused by incomplete obliteration of the omphalomesenteric duct. Occurs from bleeding mucosal ulceration. Diagnosed by technetium-99 scan which collects dye in the gastric mucosa. 2x more common in males. 2 feet proximal to the ICV. 2 inches long. Symptoms occur before 2. 2% of patients develop complications.
Intussusception – Occur with currant jelly stool in later stages. Most common cause of obstruction 6 to 36 months. Diagnosed via ultrasound. Management initially with air enema and surgery if not successful.
Milk Allergy – Painless blood in stool in an exclusively breast fed infant occurring from 2 weeks to 1 year which resolves by 18 months. Can have a cross reactivity to soy protein. Can continue breast feeding if child is growing appropriately.
Infectious Colitis – Most common cause of hematochezia across all ages. Most common pathogen causing complications is HUS O157:H7 and other shiga toxin producing E Coli. Triad of microangiopathic hemolytic anemia, thrombocytopenia, and acute kidney injury. 5-10 days of diarrhea in children < 5 years old. Early antibiotic administration may increase risk. 50% of kids who develop HUS require a period of dialysis.
Inflammatory Bowel Disease – Collection of diseases which include crohns disease, ulcerative colitis
Solitary rectal ulcer syndrome
GI Duplication Cysts
IgA Vasculitis (HSP)
Abdominal Pain – Dr. Thomas
Leading cause of ED visits 8.9% of cases
Up to 40% of patients may be discharged with a diagnosis of nonspecific abdominal pain
7% of all abdominal pain patients with life-threatening processes will present with NORMAL vital signs.
Risk is higher in elderly patients, especially with vascular causes.
History:
Abrupt onset is typically worse. Nausea / vomiting is more likely a surgical process.
Information on location and migration are useful.
Severity and description can vary greatly and has a low sensitivity and specificity.
Physical Exam:
Start in areas AWAY from where they localize the pain. Be complete.
Do not forget pelvic exam, rectal exam, or testicular exam, if required.
Imaging:
Abdominal x-rays are useful for obstruction, free air, or foreign body.
CT is often the most useful test, however is typically overused and comes with risk such as contrast reaction, cost, radiation, and difficulty managing care on a sick patient in the CT scanner.
High Risk Abdominal Pain
Visceral pain – occurs with stretching of the organs. Colicky and difficulty to localize. Ex: umbilical pain in early appendicitis
Somatic pain – Peripheral nerve pain from irritation, such as peritonitis. Better location with intense / constant pain. This is when pain associated with peritonitis or rebound pain can occur.
Referred pain – Any pain felt at a distance from the source
Elderly patients with presentation to the ED with abdominal pain have an approximately 10% mortality rate. 42% of these patients required surgery.
Hysterectomy does not require pregnancy test, however a tubal ligation always does.
UTI / Pyelonephritis increases the risk of miscarriage, however PID is rare once pregnancy is established.
Pregnant patients may have the same etiology of pain as non-pregnant patients
Always have concern for SBP in a cirrhotic patient
Paraplegic Patients
Post-operative patients with shoulder pain may be peritonitic.
CT Abdomen / Pelvis -Dr. Elsaidy
Aorta
Thrombosis
Air
Search Pattern
Respiratory Pharmacy Lecture – Zacharry Dougherty PharmD
Community Acquired Pneumonia (CAP)
Outpatient:
Azithromycin monotherapy not recommended due to local S. pneumoniae resistance rates
Clinical success is highest with cephalosporins.
Cefdinir technically has appropriate coverage, however some strains of these bacteria have resistance to this, and for this reason, it is not recommended by the ATS/IDSA
Multi Drug Resistant (MDR) Coverage:
Always consult your hospital antibiogram
Inpatient (Nonsevere vs Severe CAP):
Nonsevere:
If Prior culture, or recent hospitalization, add MRSA coverage with Vancomycin
If Prior culture, for pseudomonas change ceftriaxone to cefepime.
Severe:
Anaerobic Infections:
Room 9 Follow-up – Madelyn Huttner MD
Age 60s F found down at home confused by family with black sputum. Hx of suspected IBS. Seen initially in room 9. HR 100, BP 100/60, 94% NRB, afebrile. GCS 14, pale, dried black emesis and stool covering her body.
Orders:
Consider CTA A/P – was not obtained in this case
Medications:
Consider reversal of anticoagulation
Procedures:
Consider Minnesota tube
Anticipate significant blood in the airway
SALAD (Suction Assisted Laryngoscopy) Technique
ABG 7.3 / 29 / 45 / 14. Hgb 11.6
Na 130, K 3.2, Cl 96, BUN 46, Cr 2.2
Lactic 4.4
GI and MICU consulted from room 9. Patient found to have a history of excessive NSAID use.
Taken for emergent EGD with GI. Found to have significant esophagitis, diffusely ulcerated gastric mucosa and duodenitis.
Overview of Lithuanian Healthcare System – Simona and Deimante
Universal coverage throughout Lithuania. Patients can choose private insurance, however emergency care is fully covered. Private care is used for elective care, and faster access to care, but not common for emergency care. Can show your ID and have no-copay emergency care throughout Europe.
ED systems are based in public hospitals in major centers in Vilnius, Kaunas, and Klaipeda.
Country has a shortage of emergency medicine specialists. General practitioners are gatekeepers to other specialists.
Vilnius and Kaunas are tertiary care centers and trauma centers.
Gallbladder / Biliary Disease – Tim Price MD
30s Male with 4 days of abdominal pain. Pain is consistent and has been steadily worsening. Described as a dull pain. Located in the upper abdomen. If he lays on his back and holds his hands up, his pain is relieved. Has had regular bowel movements but has some nausea a small amount of emesis 3 days ago, as well as decreased appetite. Denies fevers or chills. Has taken hydrocodone which did help somewhat. Denies dysuria.
Differential: Cholecystitis, Choledocolithiasis, Biliary colic, Pancreatitis, Pyelonephritis, Nephrolithiasis, Hepatitis, ACS, Gastroenteritis, AAA, Cannabis hyperemesis
Labs: Elevated tbili on labs. Normal leukocyte count with neutrophil predominance
POCUS Gallbladder US: Gallstone present without pericholecystic fluid. No anterior gallbladder wall thickening. +Sonographic murphy sign.
CT – Significantly enlarged gallbladder wall
Disposition to Baptist for surgery
Rescue Task Force and Tactical Medicine – Dr. O’Brien
ABEM Certifying Exam – Dr. Platt