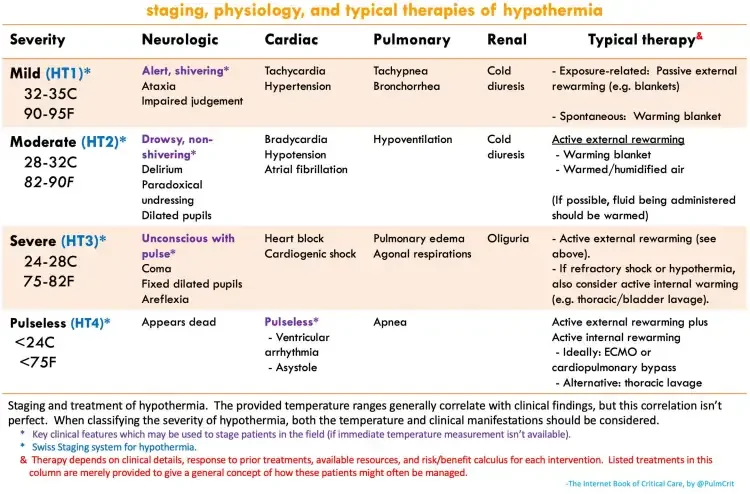
Modifications to standard ACLS algorithms in hypothermia
Medications may fail to be metabolized and accumulate. Therefore, avoid repeated doses of medications.
Defibrillation may be unsuccessful until the patient is rewarmed. Thus, serial shocks for VT/VF arrest are unlikely to add benefit. As the patient rewarms, further attempts may be made at defibrillation.
Rewarming patients with frostbite:
Goal for rapid rewarming. 40-42C is around 104-106F or about the temperature of a hot tub. This will rapidly rewarm but will not cause burns. Anything less will not rewarm tissue sufficiently. It is important NOT to rub/massage the affected digits, as the crystallized tissue is fragile and this will cause further cellular damage.
Tx: rewarm, liberal pain control, dressing/wounds care, reassess
High altitude cerebral edema (HACE) = always descend!
DERM
Rheumatic fever = Jones criteria = erythema marginatum (weeks later)
Core competencies
Interpersonal and communication skills: capacity
not competence, an informed choice, alcohol use
Level A recommendation: established evidence, multiple RCT, meta-analysis
Level B recommendation: some evidence: single RCT; multiple population
Alex Bequer, MD; Kahra Nix, MD. Peer Review Jeff Baker, MD
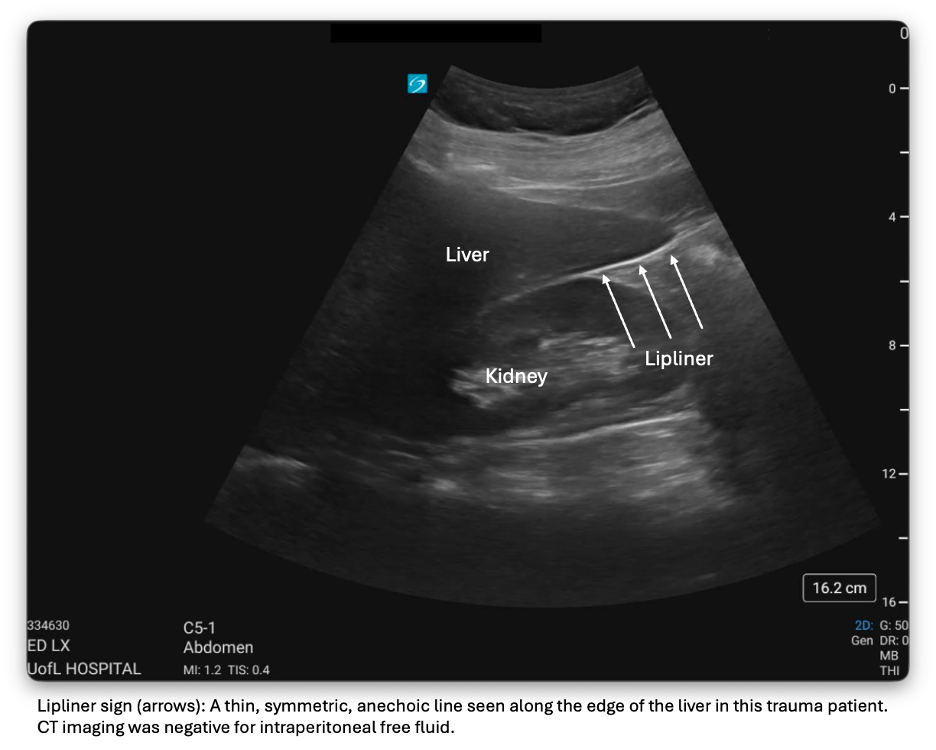
Emergency Medicine (EM) physicians are already familiar with the Focused Assessment with Sonography in Trauma (FAST) to rapidly identify intraperitoneal or pericardial free fluid and guide time-sensitive decisions. [1,2]There is an image processing error that EM physicians should be aware of as it can be confused with intraperitoneal free fluid.
Modern ultrasound machines and software increasingly strive for sharp, high-contrast images, relying on post-processing in order to improve border definition and image clarity. These adaptions are enacted to prevent speckling and result in clearer, crisp images. While these features enhance visualization, they can also introduce other limitations in image interpretation. One example is the “lipliner” which appears as a thin, symmetric, anechoic line that can be seen along the edge of solid organs (see attached image). The lipliner can be found along the caudal edge of the liver and at the splenic tip, precisely where free fluid is expected on a positive FAST examination, thereby creating the potential for false-positive interpretations. [3] Unlike true free fluid, which typically forms a wedge-shaped, dependent collection that tracks into tissue planes, the lipliner outlines the solid organ margin itself. It is a result of real-time adaptive filtering, rather than anatomy or pathology, and because it is a mathematic result, the lipliner is not technically a sonographic artifact. [3]
It is important for EM physicians to recognize and understand the lipliner. Machine vendors and POCUS leaders are working on machine presets that may preserve image quality and minimize the appearance of the lipliner. Consider looking again and adjusting probe positioning to clarify if the anechoic area is wedge-shaped and extending into potential spaces. Consider serial FAST exams. [4]
In addition to other well-known mimics of free fluid, physicians should expect to encounter post-processing errors introduced by modern ultrasound advancements designed to improve image clarity and usability. Understanding how these technologies influence image appearance is critical to accurate interpretation and informed clinical decision-making. Watch out for the lipliner when interpreting FAST scans on your next shift.
References
1. Patel NY, Riherd JM. Focused assessment with sonography for trauma: methods, accuracy, and indications. Surgical Clinics of North America. 2011;91(1):195–207.
2. Rozycki GS, Ochsner MG, Feliciano DV, et al. Early detection of hemoperitoneum by ultrasound examination of the right upper quadrant: a multicenter study. Journal of Trauma. 1998;45(5):878–883.
3. Parker MA, Hicks BG, Kaili M, et al. The lipliner sign: potential cause of a false positive focused assessment with sonography in trauma (FAST) examination. Journal of Emergency Medicine. 2024;67(6):e553–e559.
4. Ferre, R. M., & Stolz, L. A. (2025, March 13). Lipliner artifact review. American College of Emergency Physicians, Emergency Ultrasound Section. https://www.acep.org/emultrasound/newsroom/march-2025/lipliner-artifact-review
Most specific finding is a ruptured aneurysm with retroperitoneal hematoma
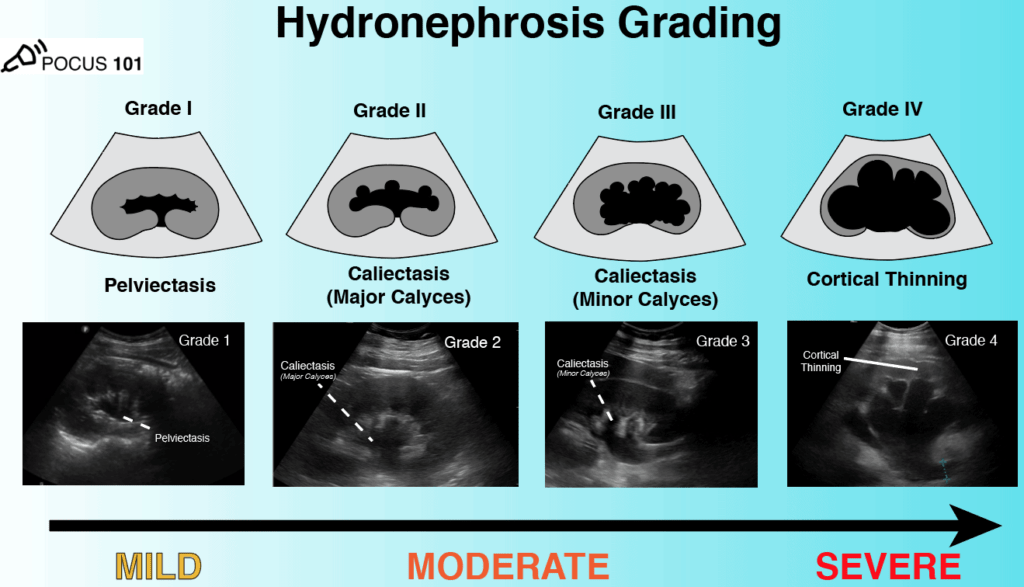
Hydroneprhosis
Cholecystitis
Measure CBD inner wall to inner wall; normal <5mm
Retinal detachment is tethered to the optic nerve
Vitreous detachment is mobile and can lead to retinal detachment
(+) HCG
Discriminatory zone 1500 IU/L
IUP confirms requires intrauterine gestational sac plus yolk sac
gestational sac alone = pregnancy of unknown anatomic location
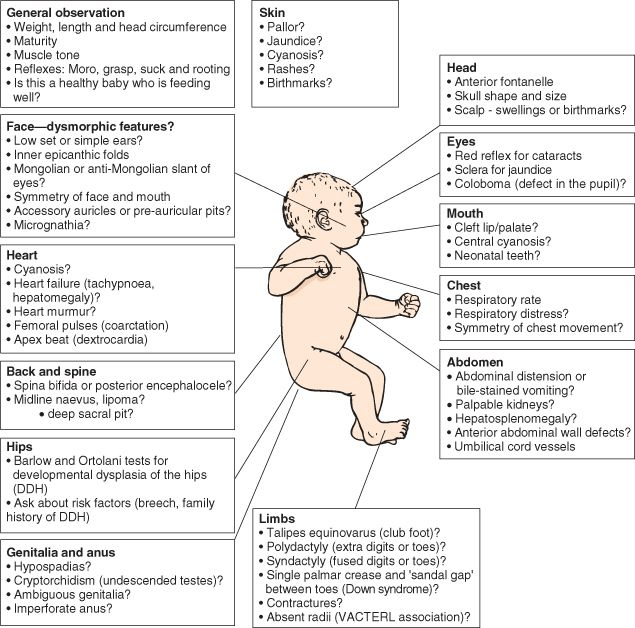
The newborn exa
examine naked and head to toe, every time (think mini trauma assessment with more steps)
Newborn well-care
The nursery
If there is suspicion you may need to tap the baby, you MUST ask about vitamin k administration
should receive hep b, erythromycin ointment to eyes, and vit k IM within 1-2 hours of birth
Feeding
newborns should take a minimum 1-2 oz of formula or breastmilk every 2-3 hous (including overnight). Normal 19 kcal/oz formula should be mixed 1 scoop of formula to 2oz of water. Water first then formula.
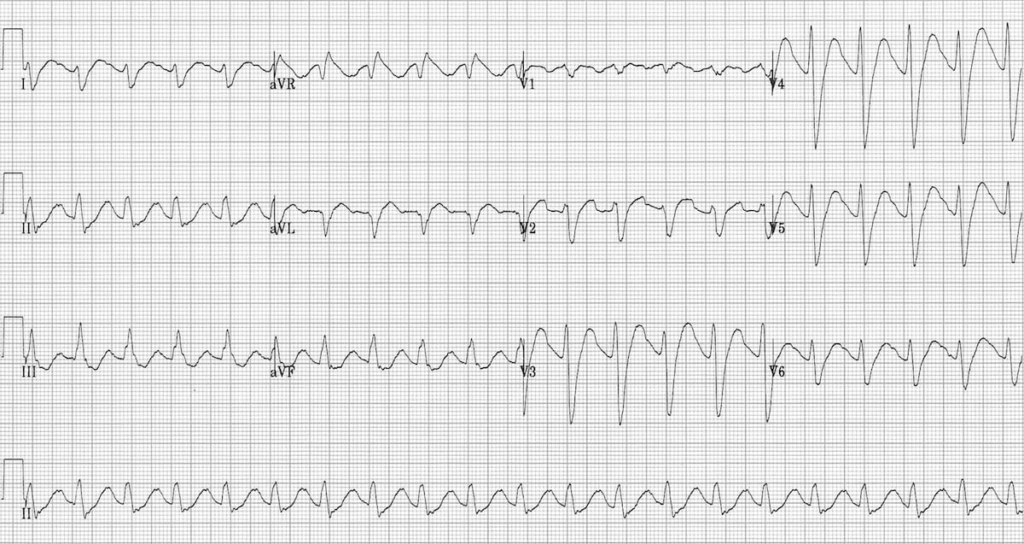
Administer IV sodium bicarbonate until you see changes in EKG
1-2 mEq/kg as intravenous push every 5 minutes as needed for termination of wide-complex tachydysrhythmia or prolonged QRS interval >120 milliseconds (ms).
![Room9er ["Room Niner"]:](https://room9er.com/wp-content/uploads/2020/03/cropped-Screen-Shot-2020-03-08-at-3.16.16-PM.png)