Most of you that have done admin work or paid attention to trends in DED, you probably have noticed that many months the majority of deaths in the ED stem from catastrophic brain damage, from both traumatic or spontaneous causes. Over 80% of my DED’s were related to severe neuro injury, so I looked at some of our common practices in handling head injuries and spontaneous bleeds and very quickly noticed that we don’t really follow any consistent patterns in caring for these folks.
Many of these patients have non-survivable injuries no matter what we do, however there are some simple interventions that might be beneficial to some cases. For instance, elevating the head of the bed >30 deg (but not more than 40) can drop ICP by 8-10mmHg, and loosening or removing an unnecessary c-collar can actually further decrease ICP by 2-5 mmHg. These are all evidence based, and while only effecting small changes, could help improve some patient’s outcomes. In addition, in discussing this with Neurosurg faculty and looking at the literature, our practice of pre-medicating head injury patients with Lidocaine is based on an old, underpowered and poorly applicable study, that used only 20 patients with known brain tumors, and is really not proven or necessary.
The following are some suggestions in dealing with Neurosurgical cases. These are practice parameters, and should be considered with every case, but this is not something that will be made standard of care, as each case should be handled appropriately at the individual physician’s discretion. However, if these interventions are not implemented, Dr. Coleman and Dr. Nauta both recommended documenting your rationale in your MDM. Also, the studies that support these practices, and some of the poorly done studies that are the basis for some of our current practices, are listed.
Increased Intracranial Pressure Protocol
Level 1
Elevate Head of Bed (30 – 40°)
Check C-collar Fit, remove as soon as possible (can ↓ ICP 2 – 5 mm/Hg, collar not necessary in isolated GSW to head, and coexistent c-spine injury rare)
Temp Normal (maintain < 98.0°F)
PaCO2 35-38 mmHg (based on EtCO2 or ABG)
Control Pain/Sedation Package if Intubated (Fentanyl)
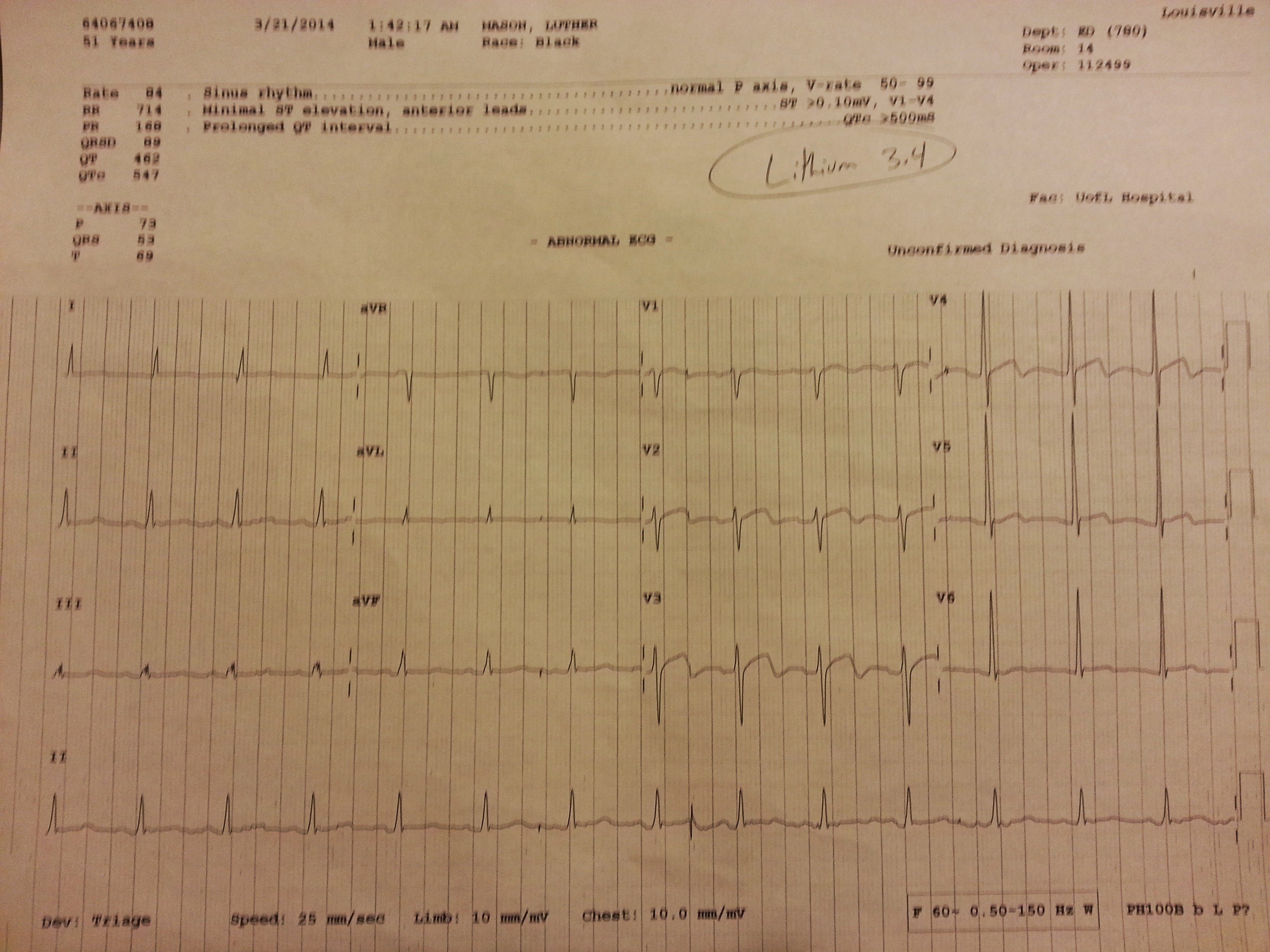
Pre-intubation Lidocaine (100mg IV) only if known tumor
Urgent Neuro Imaging
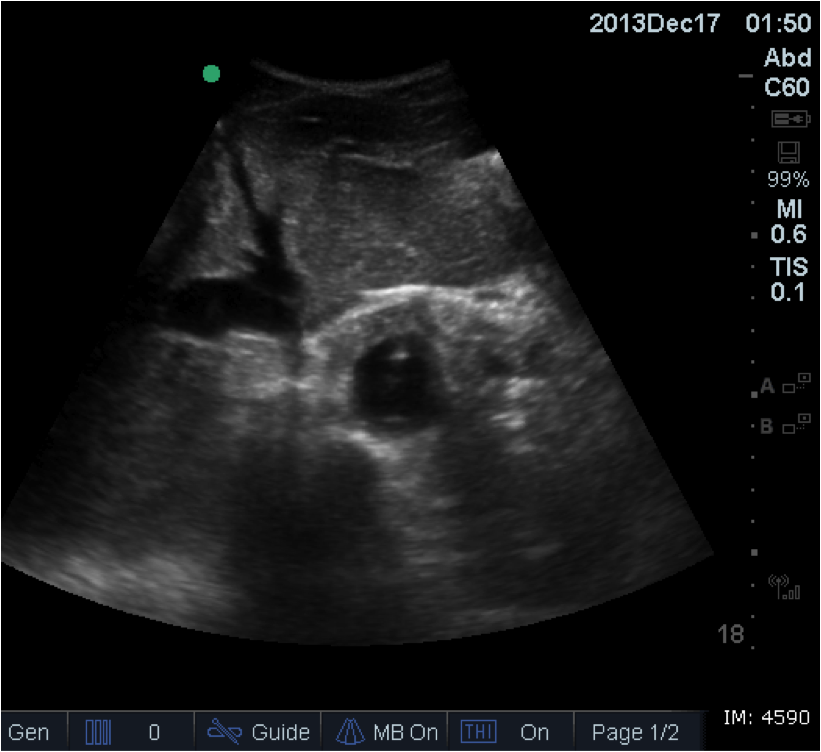
Ocular Ultrasound (Optional, do not delay definitive imaging)
Level 2 – Perform in conjunction with NES consult
Osmotic Therapy*
Mannitol – 1g/kg over 10 minutes (if hypertensive)**
Hypertonic Saline 3% – 250mL over 10 – 15 minutes (if normo or hypotensive)***
Sodium Bicarb (2 amps over 10 minutes)****
Foley catheter, replace fluid losses
Normal Saline 0.9% (No LR, D51/2NS, etc.)
Maintain Na ~ 150
Phenytoin load (15 – 20 mg/kg) only in patients with seizure or posturing
Steroids only in the case of known tumor
*Normal physiologic osmolarity range is approximately 280 to 310 mOsmol/L.
**Osmolarity of Mannitol is 550 mOsmol/L.
***Osmolarity of 3% saline is 1027 mOsmol/L
****Osmolarity of 2 amps NaHCO3 in NS is 1790 mOsmol/L
Level 3 – Perform in conjunction with NES consult, requires ICP monitoring
Propofol (or Phenobarb) gtt titrated to low levels of sedation scales (50-200 mcg/kg/min)
BIS monitoring
CPP Optimization (CPP= MAP – ICP) greater than 55 – 60
Level 4 – Only NES/NeuroAnesthesia applicable
Decompressive Craniectomy
Induced Hypothermia
Pentobarb coma (burst suppression)
Moderate Hyperventilation (Reserved as temporizing measure for patients actively herniating)
HOB
Feldman Z, Kanter MJ, Robertson CS, et al. Effect of head elevation on ICP, CPP, and CBF in head-injured patients. J Neurosurgery. 1992;76:207-211.
Ng I, Lim J, Wong HB. Effects of head posture on cerebral hemodynamics: its influences on intracranial pressure, cerebral perfusion pressure, and cerebral oxygenation. Neurosurg.2004;54:593-598.
Rosner MJ, Coley IB. Cerebral perfusion pressure, intracranial pressure, and head elevation. J Neurosurg. 1986;65:636-641.
Moraine JJ, Berre J, Melot C. Is cerebral perfusion pressure a major determinant of cerebral blood flow during head elevation in comatose patients with severe intracranial lesions? J Neurosurgery. 2000;92:606-614.
C-Collar
Stone MB, Tubridy CM, Curran R. The effect of rigid cervical collars on internal jugular vein dimensions. Acad Emerg Med. 2010 Jan;17(1):100-2.
Mobbs RJ, Stoodley MA, Fuller J. Effect of cervical hard collar on intracranial pressure after head injury. Aust J Surg. 2002 Jun;72(6):389-91.
Temp
Shiozaki T, Hayakata Taneda M, et al. A multicenter prospective randomized trial of the efficacy of mild hypothermia for severely head injured patients with low intracranial pressure.JNeurosurg. 2001;94:50-54.
Clifton GL, Miller ER, Choi SC, et al. Lack of effect of induction of hypothermia after acute brain injury. N Engl J Med. 2001;344:556-563.
Metz C, Holzschuh M, Bein T, Woertgen C, et al. Moderate hypothermia in patients with severe head injury: cerebral and extracerebral effects. J Neurosurg. 1996;85:533-541.
Marion, DW, Penrod, LE, Kelsey, SF, et al. Treatment of traumatic brain injury with moderate hypothermia. N Engl J Med. 1997; 336:540-546.
Polderman KH, Joe RTT, Peerdeman SM, Vandertop WP, Girbes ARJ. Effects of therapeutic hypothermia on intracranial pressure and outcome in patients with severe head injury. Intensive Care Med. 2002;28:1563-1573.
Resp Rate
Muizelaar JP, Marmarou A, Ward JD, et al. Adverse effects of prolonged hyperventilation in patients with severe head injury: a randomized clinical trial. J Neurosurg. 1991;75:731-739.
Newell DW, Weber JP, Watson R, Aaslid R, Winn HR. Effect of transient moderate hyperventilation on dynamic cerebral autoregulation after severe head injury. Neurosurg.1996;39:35-43.
Diringer MN, Yundt K, Videen, TO, et al. No reduction in cerebral metabolism as a result of early moderate hyperventilation following severe traumatic brain injury. J Neurosurg. 2000;92:7-13.
Muizelaar JP, Van Der Poel H, Li Z, Kontos HA, Levasseur JE. Pial arteriolar vessel diameter and CO2 reactivity during prolonged hyperventilation in the rabbit. J Neurosurg. 1988;69:923-927.
Osmotics
Smith HP, Kelly DL, McWhorter JM, Armstrong D, et al. Comparison of mannitol regimens in patients with severe head injury undergoing intracranial monitoring. J Neurosurg. 1986;65:820-824.
Khanna S, Davis D, Peterson B, et al. Use of hypertonic saline in the treatment of severe refractory post traumatic intracranial hypertension in pediatric traumatic brain injury. Crit Care Med. 2000;28:1144-1150.
Peterson B, Khanna S, Fischer B, Marshall L. Prolonged hypernatremia controls elevated ICP in head-injured pediatric patients. Crit Care Med. 2000;28:1136-1143.
Simma B, Burger R, Falk M, et al. A prospective randomized, and controlled study of fluid management in children with severe head injury: lactated ringer’s solution versus hypertonic saline. Crit Care Med. 1998;26:1265-1270.
Doyle JA, Davis DP, Hoyt DB. The use of hypertonic saline in the treatment of traumatic brain injury. J Trauma. 2001;50:367-383.
Quereshi AI, Suarez JI, Bhardwaj A. Malignant cerebral edema in patients with hypertensive intracerebral hemorrhage associated with hypertonic saline infusion: a rebound phenomenon? J Neurosurg Anesthesiol. 1998; 10:188-192.
Sedation and Paralysis
Hsaing JK, Chestnut RM, Crisp CB, et al. Early, routine paralysis for intracranial pressure control in severe head injury: is it necessary. Crit Care Med. 1994;22:1471-1476.
Temkin NR, Dikmen SS, Wilensky AJ. et al. A randomized, double-blind study of phenytoin for the prevention of post-traumatic seizures. N Engl J Med. 1990;323:497-502.
Pittman T, Bucholz R, Williams D. Efficacy of barbiturates in the treatment of resistant intracranial hypertension in severely head injured children. Pediatr Neurosci. 1989;15:13-17.
Goodman JC, Valadka AB, Gopinpath SP, et al. Lactate and excitatory amino acids measured by microdialysis are decreased by pentobarbital coma in head-injured patients. J Neurotrauma. 1996;13:549-556.
Ward JD, Becker DP, Miller JD, et al. Failure of prophylactic barbiturate coma in treatment of severe head injury. J Neurosurg. 1985;62:383-388.
Cruz J. Adverse effects of pentobarbital on cerebral venous oxygenation of comatose patients with acute traumatic brain swelling: relationship to outcome. J Neurosurg.1996;85:758-761.
![Room9er ["Room Niner"]:](https://room9er.com/wp-content/uploads/2020/03/cropped-Screen-Shot-2020-03-08-at-3.16.16-PM.png)