![Room9er ["Room Niner"]:](https://room9er.com/wp-content/uploads/2020/03/cropped-Screen-Shot-2020-03-08-at-3.16.16-PM.png)
Thrombotic Thrombocytopenic Purpura (TTP)
Pathophysiology:
- Insufficient ADAMTS-13 activity allows vWF multimers to accumulate in microcirculation which leads to platelet aggregation/thrombocytopenia and hemolysis of RBCs.
Risk Factors:
- Congenitally deficient ADAMTS-13 activity AND:
- Pregnancy OR
- Infection OR
- Inflammation OR
- Medication use (quinolones, ticlopidine, clopidogrel)
Clinical Features:
- Microangiopathic Hemolytic Anemia
- Thrombocytopenia
- Fever
- Renal pathology
- CNS abnormalities (headache, seizure, altered mental status, CVA, coma)
TTP pentad mnemonic = FAT RN
- Fever, Anemia, Thrombocytopenia, Renal, Neuro Symptoms
Workup:
- CBC with peripheral smear (anemia, microspherocytes, thrombocytopenia are suggestive findings)
- Microangiopathic hemolytic anemia produces schistocytes
- LDH (elevated)
- Haptoglobin (decreased)
- Reticulocyte count (appropriate)
- UA (hemoglobinuria)
- Creatinine (possibly elevated)
- LFT’s (increased bilirubin)
- PT/PTT/INR (normal; differentiates from DIC)
- Urine pregnancy (significant association between pregnancy and TTP)
Management:
- Heme Onc Consultation, Plasma exchange, FFP Transfusion, Glucocorticoids
Aplastic Anemia
Etiology:
- Absence or decreased number of hematopoietic precursor cells → pancytopenia (anemia, thrombocytopenia, neutropenia)
- Drug induced, viral infection, autoimmune, congenital
Presentation:
- Anemia (weakness, fatigue, dyspnea), Thrombocytopenia (mucosal bleeding, petechiae, ecchymosis), Neutropenia (recurrent infection, fever)
Workup:
- CBC (pancytopenia), CMP, Reticulocyte Count (reduced or absent), peripheral smear, LDH, Haptoglobin, consider viral serologies
Management:
- Heme Onc consultation for all new cases, especially if severe
- Transfuse PRBS/platelets as needed for severe anemia/thrombocytopenia
Angioedema
Etiologies:
- Mast cell activation/Histamine-mediated
- Allergic angioedema: IgE-mediated type I hypersensitivity
- Bradykinin-mediated
- Hereditary angioedema: Congenital or acquired loss of C1 esterase inhibitor
- Due to C1 esterase inhibitor deficiency
- Leads to unregulated activity of vasoactive mediators (bradykinin) associated with complement pathway
- Autosomal dominant
- ACE-Inhibitor induced angioedema: ACE-I adverse reaction from excessive bradykinin
- Unknown/idiopathic
Differentials: Anaphylaxis, Contact dermatitis, cellulitis, tonsillitis/uvulitis, PTA, retropharyngeal infection
Clinical features:
- Affects loose connective tissue (face/lips/throat, extremities, genitalia, bowel wall)
- Not gravitationally dependent
- Onset minutes to hours, Resolution hours to days
Workup:
- Testing not always needed, UTD recommends CBC, CMP, ESR/CRP, C4 level (c4 level +/- c1 inhibitor antigen testing used for future diagnosis, not part of ED management)
- Imaging not typically needed unless concern for concurrent dx (i.e. infection, abscess)
Management:
- General: Epi, Glucagon, TXA, FFP
- Hereditary/C1 acquired deficiency: Purified C1 inhibitor, kallikrein inhibitor, bradykinin b2, orally available Kallikrein
- FFP- can be used if other aren’t available.
Intubation strategies:
- Anticipate difficult airway, have backup available if possible
- Be prepared for being unable to oxygenate and ventilate, be ready to perform cric
- Be as gentle as possible- tissue is friable, irritation will cause more swelling.
- Consider intubation early-angioedema can surprise you and progress very rapidly.
- Consider intubation very early in post-TNKase cases, as cric could be devastating
- Digital (tactile) intubation strategy: Use the non-dominant index/middle fingers to palpate the epiglottis, directing a boujie or ETT into the trachea.
Dispo:
- No consensus on timing needed for obs. If stable need to be observed until signs of improvement. Most non-allergic angioedema does not fluctuate in severity.
- Consider admission: If partly allergic picture, high risk body part (airway), poor social situation
- Consider transfer: Low resource facilities, no advanced airway clinician except you, consider airway compromise en route (sometimes early intubation is the safest option prior to transfer)
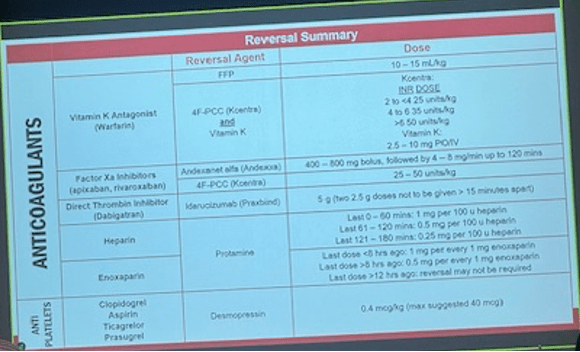
Anticoag/Antiplatelet Reversal