![Room9er ["Room Niner"]:](https://room9er.com/wp-content/uploads/2020/03/cropped-Screen-Shot-2020-03-08-at-3.16.16-PM.png)
Padget
Alcoholic ketoacidosis
Presents; n, v, dehydration, ams
Suspect in poor po + alcoholism
Alcohol increases NADH/NAD+ = higher ketones and lactic acidosis
- Malnutrition presents compensation
- p/w other metabolic derangements
Dx overlaps to some degree w starvation ketosis, DKA
- Correlate clinically
Tx
- Thiamine (WK)
- Fluids
- D5LR preferred, thiamine before
- Can treat glucose >250 w insulin
- Supportive care otherwise
- Beware CIWA
If lactic >4 something else going on
Disposition; resolution in symptoms, acidosis = home
Rizzo; small group
Case 1 – HyperK
- Ddx; medicines, renal disease, diet, rhabdo
- Ekg changes, spectrum, peaked t wave – prolonged qrs – sinusoidal
- Tx, insulin, glucose, Ca, lasiks, albuterol, fluids, dialysis
- Ca
- Gluconate through PIV
- Chloride in codes, central lines
- Dialysis
- K refractory to treatments
- Ca
Case 2 – HypoK
- Ekg changes – U waves
- Ddx; diet, DM, GI loss, medicines
- Tx;
- Mg, repletion
- K repletion
- 10meq = .1 increase
Case 3 – HypoNa
- Ddx; Polydipsia, SIADH, polypharm, CKD, aldosterone deficiency
- Tx; Replete w hypertonic 150mg / 10-20min
- Can use x2-3 amps bicarb
- <120 = ICU
- Don’t correct too quickly
Case 4 – HyperCa
- Ddx; exogenous, PTH, genetic disorder, bone resorption, addison, pagets, malignancy, polypharm
- Tx; Fluids, supportive, Ca binders, bisphos, dialysis
- EKG changes = osborne J wave, shortened QT
Case 5 – HypoMg
- Ddx; malnutrition, alcohol, gi loss, renal loss
- Ekg changes – prolonged qtc, risk for ventricular arrhythmia
- Tx; replete
- Beware of rapid infusion – respiratory depression, hyporeflexia, hypotension
Ross; Small group
Case 1 – thyroid storms
- Precipitant; trauma, infection, contrast, medicines
- Burch and Wartofsky score to sound smart to endocrinology
- Tx
- Ptu vs methimazole (avoid in 1st trimester pregnancy)
- Propranolol vs esmolol (beta selective)
- Iodine, can substitute Li if allergic
- Steroid
- Cholestyramine
- Avoid, amio, asa
Hashimoto – low thyroid
Exogenous – dont need ptu, methimazole
Case 2 – HTN emergency (pheo)
- Ddx; pheochromocytoma, substance use, idiopathic, kidney disease, carcinoid, angina
- If pheo/cocaine avoid beta blockade
- Plasma metanephrines for pheo, urine catacholamines
- Tx;
- Phentolamine
- Oral doxazosin if stable
- Cardine
- Nitroprusside
- Imaging – CT scan w adrenal protocol
- Associated w MEN2, neurofibromatosis, von hippel lindau
- Reglan, TCA, steroids can exacerbate
- Common sx; palpitation, diaphoresis, HA
Case 3 – Myxedema coma
- Ddx; hypothermia, sepsis, chf, trauma, renal
- Tx;
- Levothyroxine, consider T3 too (if TSH> 10)
- T4 preferred in old people, significant CAD
- Hydrocortisone if c/f concomitant adrenal insufficiency
- Passive rewarm
- Beware of pericardial effusion – low voltage ekg
- Get an echo
- Levothyroxine, consider T3 too (if TSH> 10)
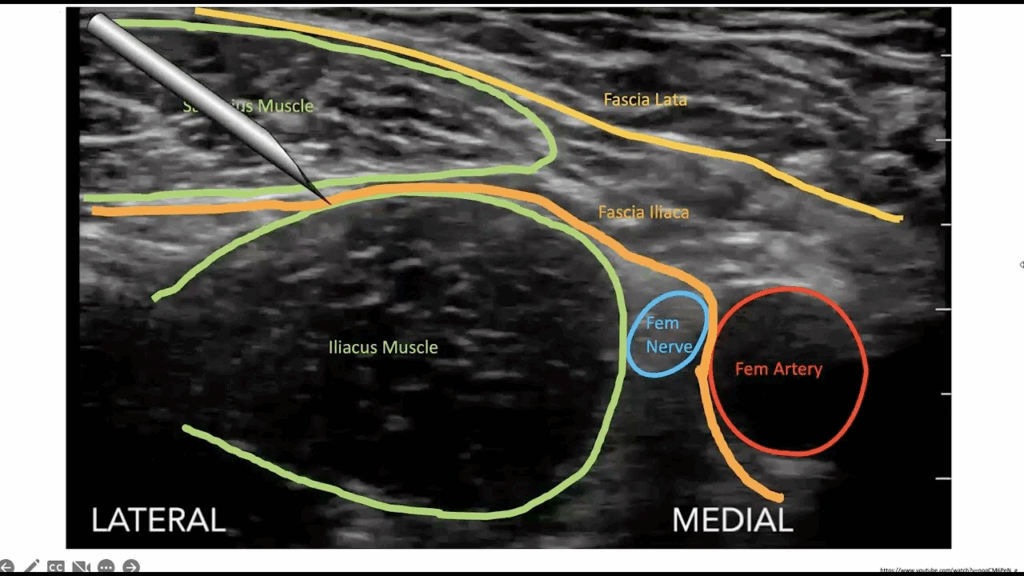
Bequer/Baker; US
Fascia Iliaca Block
Blocks femoral/obturator/lateral cutaneous nerves
Indications
- femoral head/neck/trochanter fractures
- Anterior thigh lac/abscess
Careful on anticoagulated pts
Ropivicaine/bupivicaine preferred (longer acting)
Use linear probe
2 person procedure
- X2 syringe
- Threeway stopcock
Enter laterally between fascial planes