![Room9er ["Room Niner"]:](https://room9er.com/wp-content/uploads/2020/03/cropped-Screen-Shot-2020-03-08-at-3.16.16-PM.png)
Rheumatic Fever
Pathophysiology:
- Inflammatory disease occurring 2–4 weeks after an untreated group A strep infection (strep throat or scarlet fever), primarily affecting children aged 5–15
- Connective tissue of heart, joints, CNS, subcutaneous tissues are targeted by immune reaction
Clinical Features:
- Polyarthritis, pericarditis, Sydenham’s chorea, erythema marginatum, nodules
Workup:
- CMC, CMP, ESR, CRP
- ASO (Antistreptolysin O) titer Elevated 1week to 1 month after GAS infection
- Anti-DNase B titer is elevated longer than ASO and may be useful for patient presenting later than 2-4 months or with a negative ASO
- ECG – Looking for prolonged PR or other AV block
- CXR
- Echocardiogram
Management:
- Eliminate underlying streptococcus bacteria with antibiotics (penicillin), reducing inflammation, pain, and fever with aspirin or other NSAIDs. Consider corticosteroids for heart inflammation.
- Long-term, secondary prevention with regular antibiotic injections (Penicillin G IM x1 month) to prevent recurrence and heart damage
Tumor Lysis Syndrome
Overview:
- Occurs when large numbers of cancer cells die and release their contents into the circulatory system
- Usually with onset of new chemotherapy or high tumor burden.
- -K, Phosphate, calcium, nucleic acids -> urine acid, proteins
- Can lead to AKI and renal failure
- Usually within 72 hours, can have later presentation up to 10 days (i.e.. Immune checkpoint inhibitors)
- Laboratory or clinical diagnosis
Risk factors:
- Cancer type (NHL, Lymphoma, AML, and ALL most common).
- Solid tumors with high tumor burden
- Age, kidney function, dehydration, renal and CNS involvement, presence of mediastinal mass, LDH >2x upper limit of normal indicates rapid cell turnover
Clinical Presentation:
- Nonspecific, commonly involved the renal, neurological, and cardiac systems
- Trousseau-muscle spasm with inflation of BP cuff = hypocalcemia
Workup:
- CBC, CMP, Phosphorus, Calcium, Uric Acid, LDH, EKG, UA
- Cairo-Bishop Diagnostic Criteria
Management:
- Treat electrolyte derangements, IVF (2-3x maintenance fluid dose), manage uric acid (rasburicase or allopurinol)
- Consult Heme Onc, Renal
- Likely admit
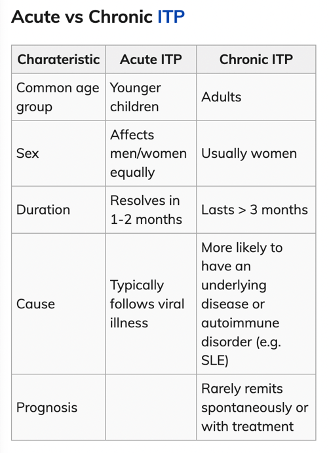
ITP (Immune Thrombocytopenic Purpura) Case
Overview:
- Immune mediated destruction of platelets
- Primary (idiopathic) vs Secondary (part of larger pathology or medications)
- Presentation: Petechia, purpura, epistaxis, gingival bleeding, mouth lesions, acute bleeds
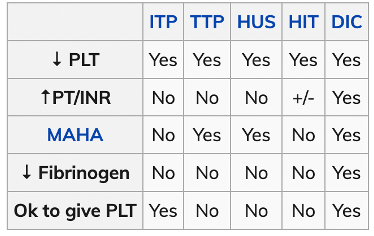
- Thrombocytopenia plt < 100 with no change in other cell lines
- Need to differentiate between others (ITP, HIT, HUS, TTP, DIC)
Treatment:
- Minor OR Platelet < 30: Dexamethasone 40 mg IV
- Severe: Dexamethasone 40 mg IV, IVIG 1g/kg, Plt transfusion (goal 50-100), splenectomy?
- Treatment same in pregnant patients and pediatrics.
Diving Medicine
Key History to Obtain:
- Dive depth
- Dive duration
- Number of dives
- Ascent rate
- Safety stops performed
- Time since surfacing
- Air source
- Prior dive illness
- Look at diving watch to obtain this data quickly
1. Decompression Sickness (DCS)
Related to nitrogen bubble formation during ascent.
Mechanism:
- Increased pressure underwater dissolves nitrogen into tissues.
- Rapid ascent → nitrogen comes out of solution → bubbles form in blood/tissues.
Types:
Type I (Mild)
- Musculoskeletal pain (“the bends”)
- Joint pain (shoulder, elbow, knee most common)
- Skin findings
- Pruritus
- Mottled rash (cutis marmorata)
Type II (Severe): Involves neurologic, pulmonary, or vestibular systems
- Weakness
- Paresthesia
- Paralysis
- Ataxia
- Bladder dysfunction
- Confusion
- Vertigo
- Hearing loss
Pulmonary form (the chokes):
- Chest pain
- Cough
- Dyspnea
Diagnosis: Recent dive (usually within 6–24 hours), Compatible symptoms
Treatment:
- 100% Oxygen
- IV fluids
- Supine positioning
- Immediate hyperbaric consultation
- Recompression therapy
Hyperbaric therapy dramatically improves outcomes.
2. Arterial Gas Embolism (AGE)
Most dangerous diving emergency.
Mechanism
- Rapid ascent → lung overexpansion → alveolar rupture
- Air enters pulmonary veins → systemic embolization
Presentation (often within minutes of surfacing)
Neurologic symptoms:
- Stroke-like deficits
- Seizures
- Altered mental status
- Paralysis
- Vision changes
Other symptoms:
- Chest pain
- Dyspnea
- Cardiac arrest
Treatment:
Same as severe DCS:
- 100% Oxygen
- Hyperbaric recompression (urgent)
- IV fluids
3. Barotrauma
Occurs when air spaces cannot equalize pressure.
Ear Barotrauma (Most Common)
-Severe ear pain with descent. If ears are not equalized, pressure builds and eustachian tube collapses. Clear ears on water entry and often during dive.
Symptoms:
- Ear pain
- Hearing loss
- Vertigo
- TM rupture
Exam:
- Hemotympanum
- TM perforation
Treatment:
- Analgesia
- ENT follow-up
- Avoid further diving
- Give antibiotics only for perforated TM
Sinus Barotrauma
Symptoms:
- Facial pain
- Epistaxis
- Sinus pressure
Treatment:
- Decongestants
- Analgesia
Pulmonary Barotrauma
Causes:
- Pneumothorax
- Pneumomediastinum
- Arterial gas embolism
Symptoms:
- Chest pain
- Dyspnea
- Subcutaneous emphysema
Treatment:
- Manage pneumothorax
- Oxygen
- Hyperbaric if embolism suspected
4. Nitrogen Narcosis
Occurs at depth >30 meters (~100 ft).
Symptoms:
- Euphoria
- Poor judgment
- Confusion
- Impaired coordination
Treatment:
- Ascend to shallower depth
Symptoms resolve quickly, it is safe to continue diving after resolution of symptoms.
Immediate ED Management
- High-flow oxygen
- IV fluids
- Neurologic exam
- Call hyperbaric center
- Transport if needed
In the U.S., consultation is often through:
- Divers Alert Network, they assist with hyperbaric referral and organizing transfer
Board Pearls
- Any neurologic symptom after diving = assume AGE or DCS → hyperbaric therapy
- Symptoms within minutes of surfacing → think AGE
- Symptoms hours later → think DCS
- Joint pain after diving = DCS Type I
- Stroke-like symptoms after diving = AGE until proven otherwise
Immunosuppression and Transplant
Common ED patients:
- Solid organ transplant
- Bone marrow transplant
- Chemotherapy
- Chronic steroids
(>20 mg prednisone daily for >2 weeks) - Advanced HIV
- Biologic therapy
Common immunosuppressive drugs:
- Typical regimen includes: calcineurin inhibitor + antimetabolite + steroid
- Calcineurin inhibitor (Cyclosporine, Tacrolimus)
- Steroids
- +/- Antimetabolite (Azathioprine, Mycophenolate mofetil)
Solid Organ Transplant Rejection:
- Hyperacute (Minutes–hours)
- Acute Rejection (Weeks–months)
- Chronic Rejection (Months–years)
Organ-Specific Rejection Clues:
Kidney Transplant:
- Rising creatinine
- Decreased urine
- Hypertension
Liver Transplant:
- Fever
- RUQ pain
- Elevated LFTs
- Jaundice
Heart Transplant:
- Dyspnea
- Heart failure symptoms
- Arrhythmias
- Because transplanted hearts are denervated, they may NOT present with typical chest pain.
Neutropenic Fever:
- ANC <500 OR <1000 with predicted nadir of <500 in 48h AND
- Fever ≥ 38.3˚C (100.9˚F) once OR sustained temperature ≥38 (100.4) for >1hr