![Room9er ["Room Niner"]:](https://room9er.com/wp-content/uploads/2020/03/cropped-Screen-Shot-2020-03-08-at-3.16.16-PM.png)
TCA Toxicity (Marks)
- Most Common Use for MDD, Neuropathic pain
- 3% of antidepressant overdoses but 20% of deaths
- Toxicity most typically seen within 2-6 hours of ingestion
- Most commonly presents as anticholinergic syndrome
- Workup: Tox, TCA level, BMP, VBG, EKGs (looking for QRS>100ms)
- Tx: Sodium Bicarbonate (1-2 mEq/kg rapid IVP, repeat, stop pH > 7.50-7.55)
- NEVER USE PHYSOSTIGMINE (can cause lethal bradyarrhythmia)
- For Seizure: 1) Benzos, 2) Barbituates/Propofol
- For Hypotension: 1) IVF boluses, 2) Norepi
- Asymptomatic: Observe 6 hours, discharge
- Symptomatic patient: high suspicion: floor vs ICU regarding presentation
- Eisenstat Pearl: Aggressive bicarb early on
Salicylate Toxicity (Hudson)
- Typically presents as Delirium, GI symptoms, Tinnitus,
- Found in Aspirin, Oil of wintergreen, maalox, pepto bismol, wart removers
- Uncouples oxidative phosphorylation → increased metabolic rate and hyperthermia
- Toxic Dose= 150 mg/kg, Minimal lethal dose 450 mg/kg
- Triple-Mixed Acid Base Disturbance: Resp Alk, AG Metabolic Acidosis, Met Alk
- Workup: ASA, Acetaminophen, CMP, Mag, Phos, UA, VBG, EKG, Tox
- Airway: Avoid intubation unless absolutely necessary, difficult to achieve adequate minute ventilation on vent. Give bicarb prior to intubation
- Breathing: Acute lung injury leads to higher O2 requirements
- Circulation: Hypotension common due to systemic vasodilation, Tx IVF/pressors
- Decontamination: Charcoal, WBI
- Dialysis: For AMS, Sz, Pulmonary Edema, Hypoxemia, pH<7.20.
Heavy Metals (Eisenstat)
- Metals EM Docs Need to Know- Iron and Lead
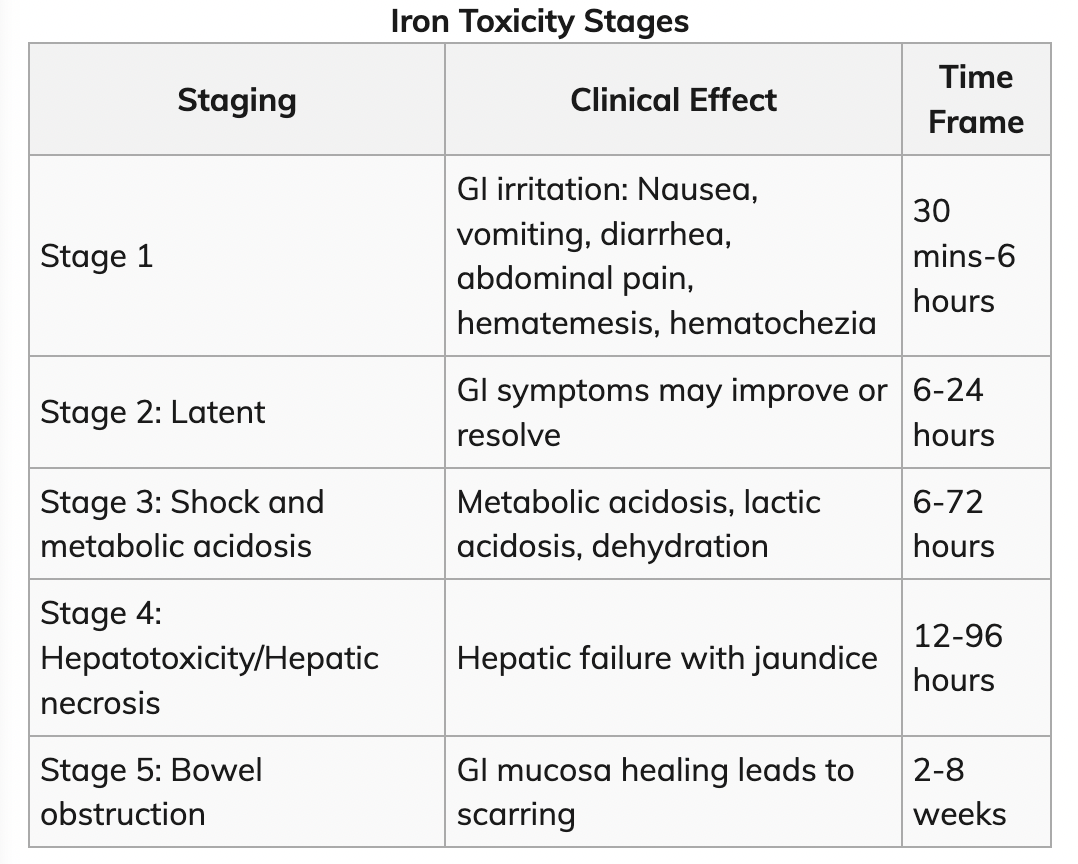
Iron
- Used therapeutically in various remedies for thousands of years
- Literally impossible to get iron toxic from normal dietary sources
- In Overdose, oxidative effects irritate GI lining
- Drops cardiac inotropy, Combination of fluid loss, Multisystem organ dysfunction, Leads to Acidosis, shock
- Workup: Iron Level (don’t worry about TIBC/ transferrin)
Answers to Know for Poison Control Center Consult
- Time and ingestion
- Form and amount
- Serum iron level (& how long from ingestion)
- pH, lactic acid
- Symptoms
- Imaging (Abd XR)
- Treatment: Activated charcoal doesn’t work, Consider WBI, endoscopy
- Deferoxamine- binds up serum iron and lets you pee it out (5 mg/kg/hr increase to 15 mg/kg/hr)
- Side Effects: Can cause hypotension, ARDS, yersinia infections, Vin Rose urine
Lead
- No safe lead level
- Phased out of gasoline and paint in 1970s
- Toxicity rare in US
- Most common presentation is peds patient sent by PCP who is asymptomatic
- Screening in US done in Medicaid patients, high risk cities, immigrants
- Workup: Send venous blood lead level
- Treatment: Succimer, Calcium EDTA, BAL aka Dimercaprol
- Removing source-talk to health department, remediation of house, surgical removal of bullets
Altitude Sickness (Ganshirt)
Spectrum of diseases caused by too rapid of ascension, inadequate time to adjust to changes in O2 and atmospheric pressures
Acute Mountain Sickness
- Mechanism- We don’t know exactly
- Headache, nausea vomiting fatigue
- Older individuals are less likely to get this (less fit, don’t ascend as fast?)
- Treatment- immediate descent, Dexamethasone vs acetazolamide
- How to Avoid: Slow pace of ascent, Avoid alcohol, Hike day before to get used to partial pressures
- Acetazolamide as prophylaxis for those with history but it has side effects
HACE- High altitude cerebral edema
- Potentially fatal
- Mechanism- vasogenic vs cytotoxic edema
- Signs: AMS, ataxia, gait disturbance, stupor
- Tx- IV dexamethasone, hyperbaric for severe cases
- Prevention- acclimation, Diamox
HAPE- High Altitude Pulmonary Edema
- Mechanism- Heterogeneous pulmonary vasoconstriction
- Tx- slow descent, Supplemental O2, nifedipine gtt
- Nifedipine- reduction in pulmonary artery pressure
- Prevention- acclimation, slow ascent, nifedipine/sildenafil
- Nifedipine is effective prophylaxis in patients with prior episodes of HAPE
Decompression Illness
- Mechanism- pressure driven problem
- Presentation-organ system based
- Treatment- 100% FiO2, Hyperbaric O2
- Prevention- Slow ascent, avoid plane rides home for 24 hours
Hypothermic Cardiac Arrest (Edwards)

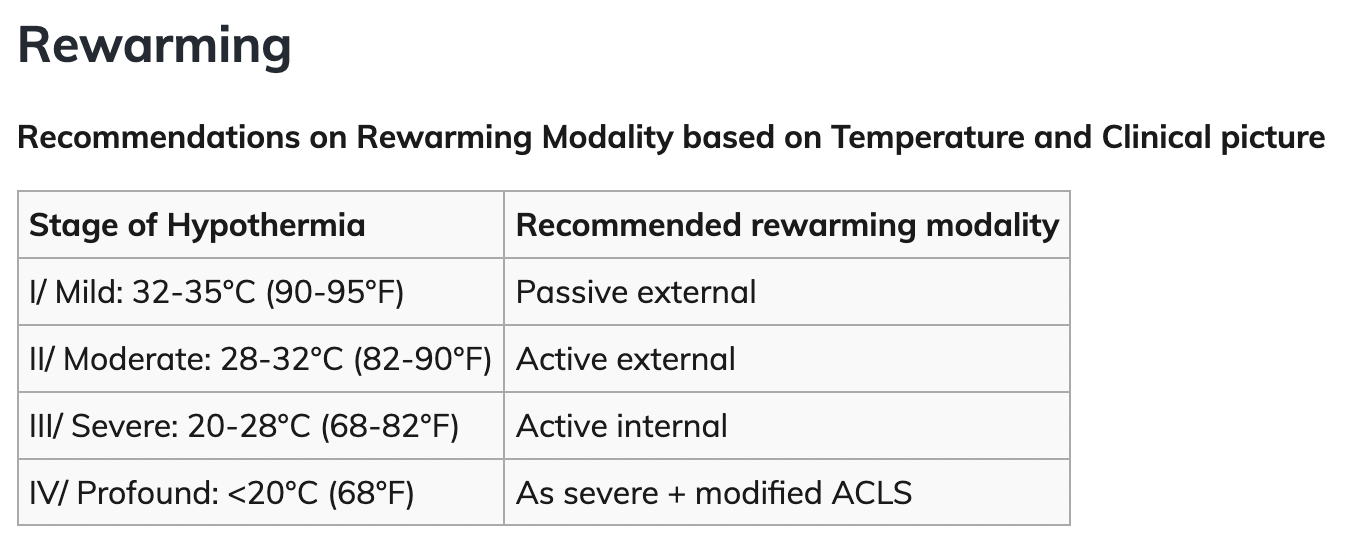
Passive External- Remove wet clothes, heated room, blankets
Active External- Heated blankets, bair hugger/ arctic sun, warm humidified air/02
Active Internal- Heated IVF, Bladder and thoracic lavage, ECMO, peritoneal lavage (not here)
ACLS
- ERC guidelines: up to 3 defibrillations with epi held until temp >30C, then epi q6min until temp > 35C
- AHA guidelines: 3 defibrillations and 3x epi with further dosing guided by response
Termination of CPR
- K > 12
- Asystole persists beyond >32 C
- MUST BE WARM AND DEAD
Outcomes
- Impressive outcome statistics
- WITNESSED hypothermic arrest: approx 73% survival to discharge and 89% of survival with favorable neurologic outcomes
*Screenshots of charts taken from WikiEM.*