![Room9er ["Room Niner"]:](https://room9er.com/wp-content/uploads/2020/03/cropped-Screen-Shot-2020-03-08-at-3.16.16-PM.png)
HPI: 57 yo M w/ PMHx of HTN, HLD presents with concern for carbon monoxide poisoning. Pt reports he was using a gas-powered saw in an enclosed bathroom to cut concrete. After some time, he began to feel hot and dizzy. When he stood up to walk out of the bathroom, he reported being unable to walk straight. He then began to feel lightheaded and developed a headache. He has also developed photophobia since. He reports no other problems. Smokes approximately 1ppd.
Exam: Vital Signs WNL
GEN: Alert, with no distress
CV: RRR, S1S2 present, No M/R/G
Pulm: CTAB, Non-labored
Neuro: CN II-XII intact, Strength 5/5 in all extremities, Normal Sensation/Coordination
Labs: CarboxyHb lvl 19.3%
ABG showed normal pH, pCO2, pO2, Bicarb
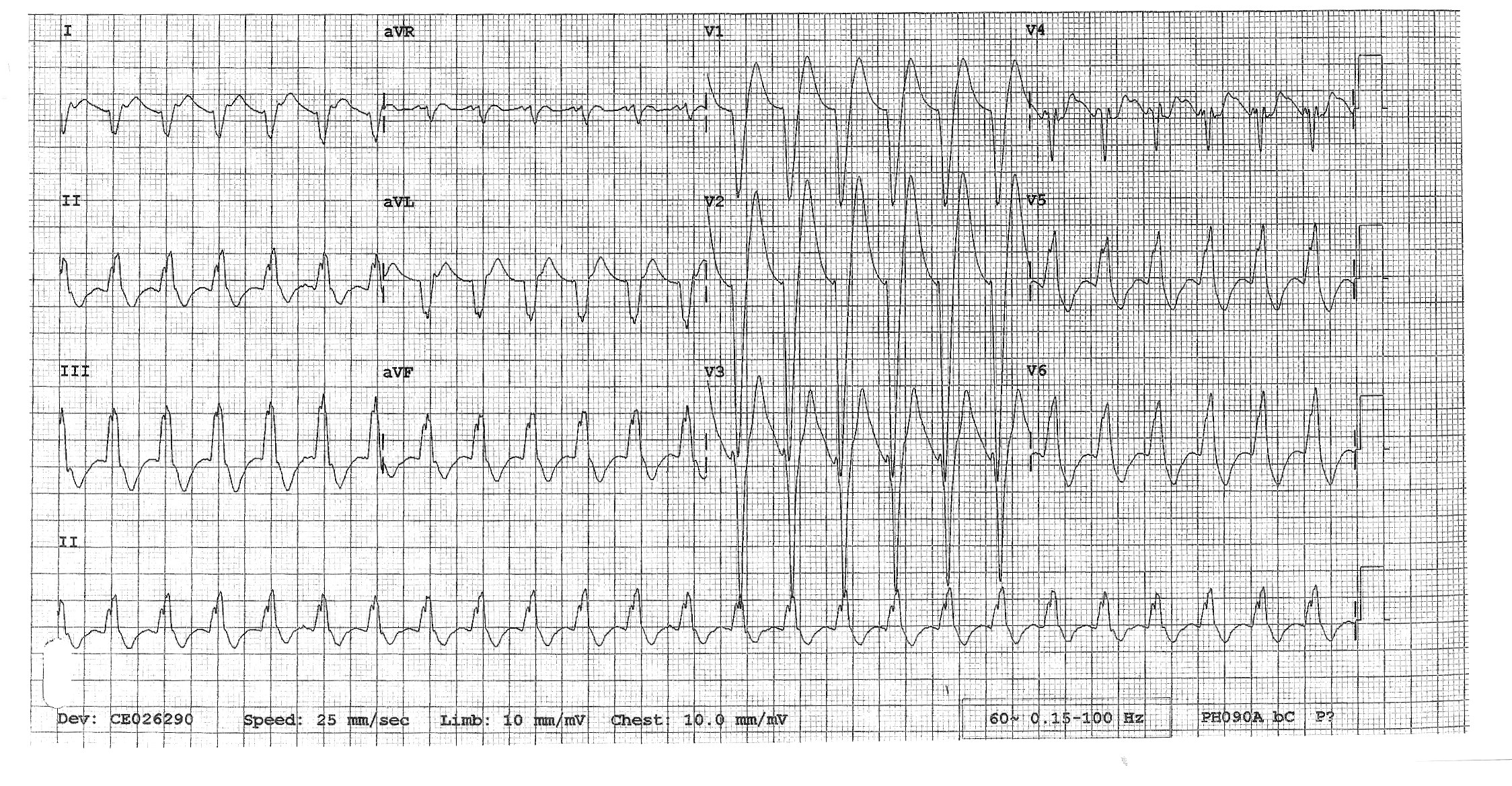
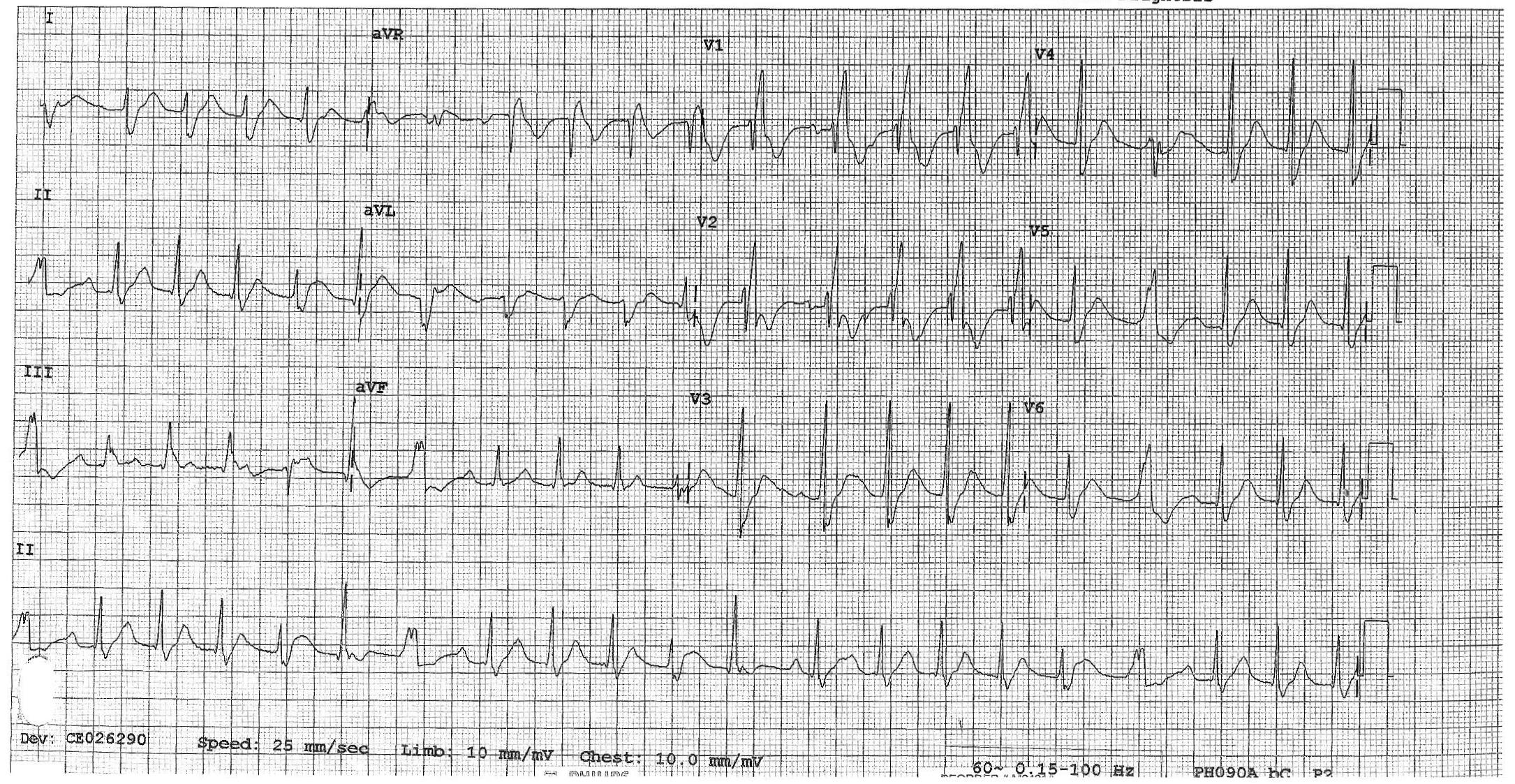
CBC, CMP, Troponin, EKG, and CXR negative for acute process
Dispo: He was placed on a NRB and symptoms began improving. After discussion with Poison Control and Jewish, pt was transferred to Jewish to receive a hyperbaric O2 treatment. He felt much improved after the treatment and was discharged in good condition.
The suspicion for carbon monoxide poisoning is based primarily on history. Most symptoms are non-specific. Mild to moderate CO poisoning presents with headache (most common), nausea, dizziness. Don’t forget to ask about LOC. Severe CO toxicity can produce neurologic symptoms (seizures, syncope, or coma) and/or end organ damage. If CO toxicity is suspected based on history, a careful and detailed neurologic exam should be performed.
If sufficient concern after history and physical, the diagnosis is made by an elevated carboxyhemoglobin level measured off an arterial blood gas sample. Nonsmokers should have baseline level of less than 3% carboxyhemoglobin. Smokers may have baseline levels of 10-15%. Once the diagnosis of CO poisoning is confirmed, an EKG should also be performed. CMP should also be considered to evaluate for electrolyte abnormalities and to assess renal function. Troponin should be obtained in patients with EKG abnormalities, cardiac comorbidities, and older patients.
CO binds hemoglobin with greater affinity than oxygen. This results in impaired oxygen transport. CO can also precipitate an inflammatory cascade that results in CNS lipid peroxidation and delayed neurologic sequelae. The half-life of CO can be changed by manipulating O2 delivery to the patient. CO half-life is approximately:
· 250 to 320 minutes on room air
· 90 minutes on high-flow oxygen via a NRB face mask
· 30 minutes with 100 percent hyperbaric oxygen
Some evidence suggest that HBO treatment can decrease the chance of delayed neurologic sequelae. Patients can often be discharged soon after HBO treatment is completed.
Recommendations for Hyperbaric Oxygen from Rosen’s 9E:
· Carboxyhemoglobin (COHb) independent of clinical findings
o >25% with no clinical findings
o >15% in pregnancy or fetal distress
· Or an elevated COHb with one or more of the following findings:
o Syncope
o Coma
o Seizure
o Altered mental status (GCS <15) or confusion
o Abnormal cerebellar function
o Prolonged CO exposure with minor clinical findings
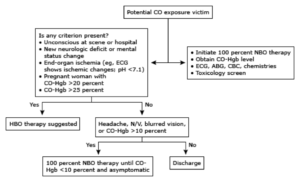
Suggested treatment algorithm from UpToDate:
References:
Walls, Ron M., et al. “Inhaled Toxins.” Rosen’s Emergency Medicine: Concepts and Clinical Practice, Elsevier, 2018.
Clardy, Peter F, et al. “Carbon Monoxide Poisoning.” UpToDate, 28 Feb. 2017, www.uptodate.com/.