![Room9er ["Room Niner"]:](https://room9er.com/wp-content/uploads/2020/03/cropped-Screen-Shot-2020-03-08-at-3.16.16-PM.png)
Infective Endocarditis Lightning Lecture
- Pathophysiology: Usually starts with an insult to the endothelium, leading to formation of sterile vegetations. Then, an episode of transient bacteremia may seed an infection to these pre-existing vegetations
- Infected vegetations often embolize, leading to a wide range of symptoms and secondary effects
- Prevalence is as high as 10-15% in those who abuse IV drugs
- The Modified Duke Criteria is used for diagnosis
- When you suspect IE, three blood cultures from three different sights should be drawn
- Antibiotic selection varies depending on native or prosthetic valve
Pericarditis and Myocarditis Lightning Lecture
- Myocarditis is inflammation of the muscle cells of the heart. Can be acute, subacute or fulminant
- Wide range of etiologies including viral/ bacterial infections and autoimmune diseases
- Can lead to dilated cardiomyopathy and heart failure
- Up to 80% of cases of pericarditis have an idiopathic etiology. Other causes include infections, radiation, Dressler’s syndrome
- Pericarditis can lead to effusions/ adhesions, leading to constrictive pericarditis or even tamponade
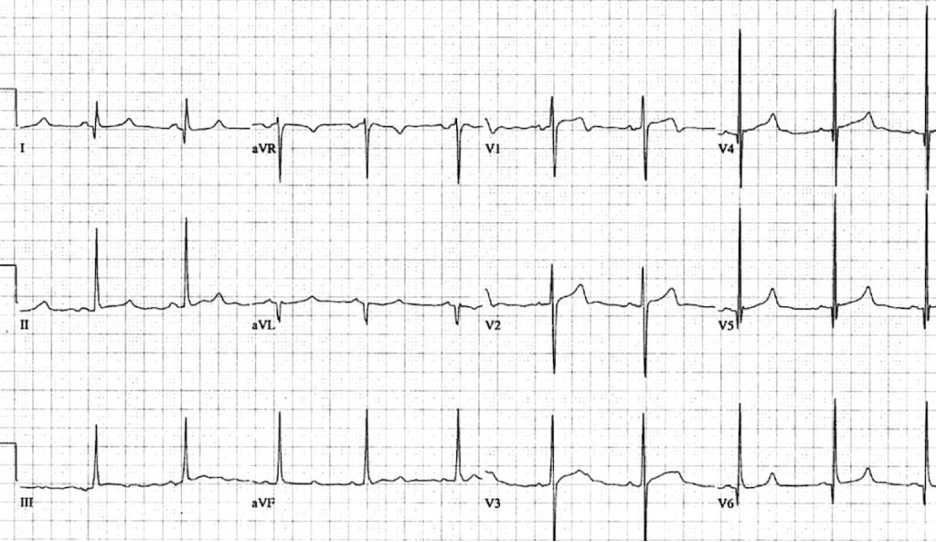
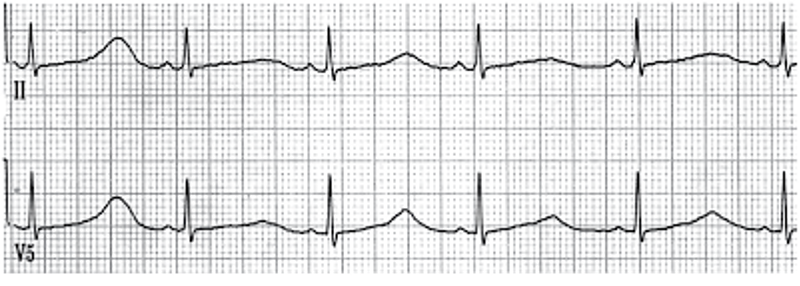
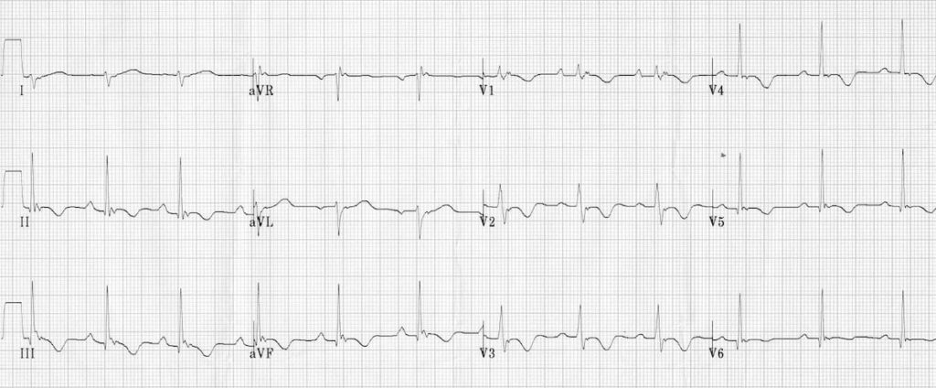
- Pericarditis does have some characteristic EKG findings. Important to differentiate from a STEMI
Pediatric Congenital Heart Disease
- CHD is the most frequently occurring birth defect
- Cyanotic lesions- think the “Five T’s” plus pulmonary atresia
- When you’re concerned about a ductal-dependent lesion, don’t hesitate to give prostaglandins; biggest side effect is apnea, which can be managed
- First two things to get when a newborn presents with suspicion of a CHD: All four extremity BPs and preductal+ postductal O2 sats
- First two things to do during a suspected tet-spell: Squat/ knees to chest and give O2
- If a baby is tachycardic, try to address potential secondary causes before giving adenosine
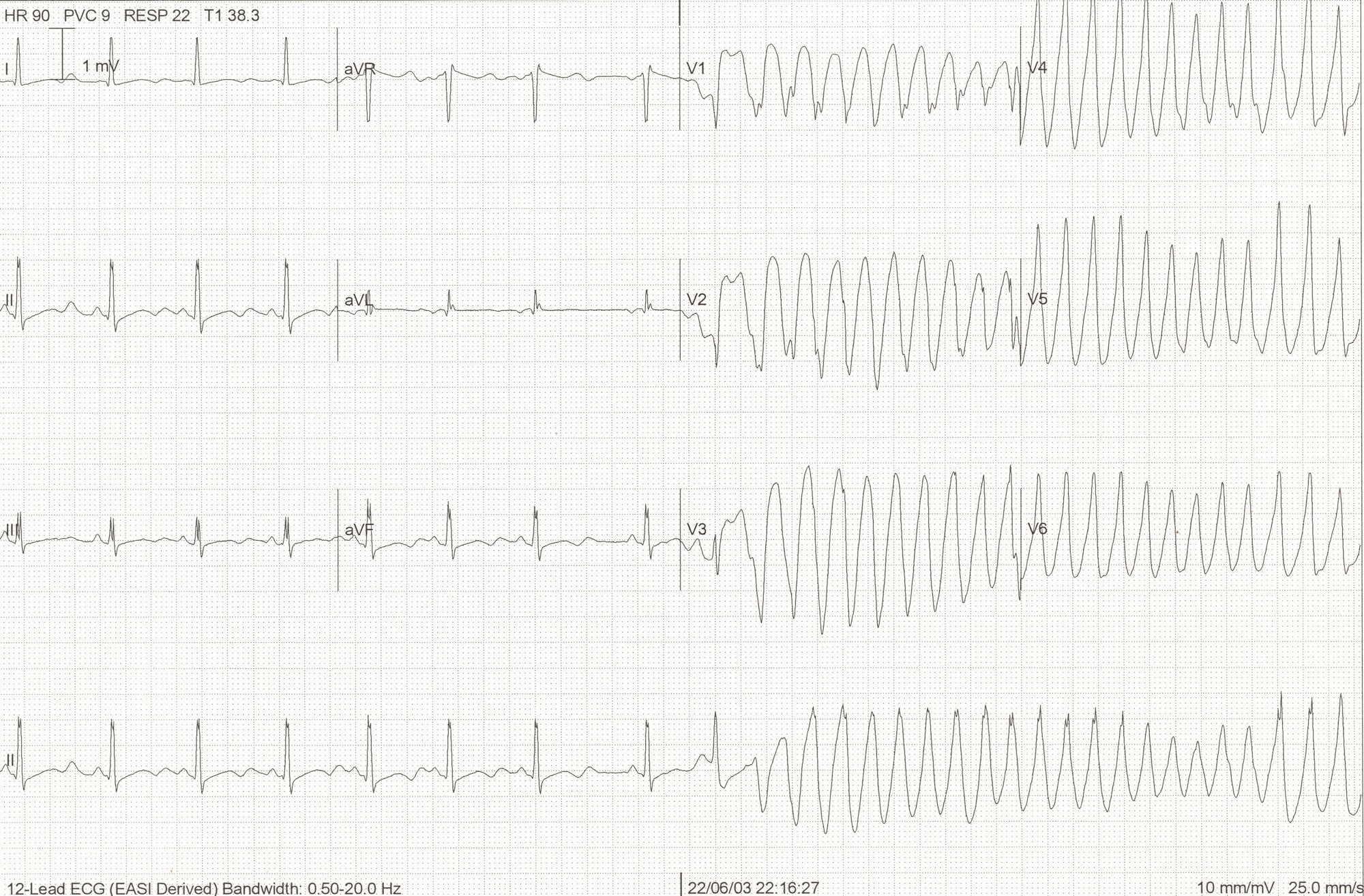
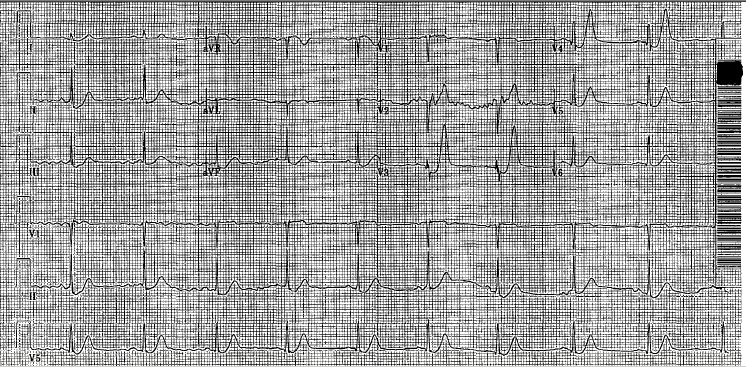
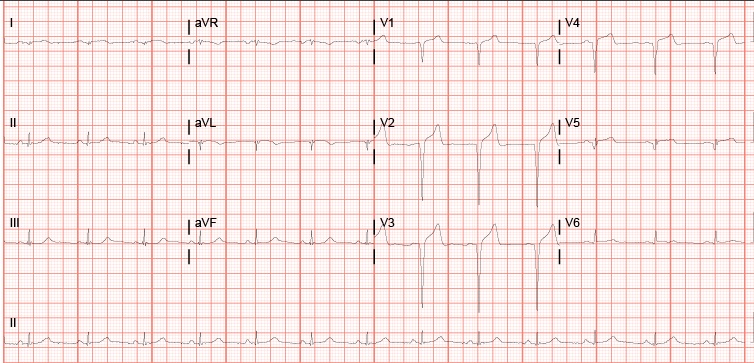
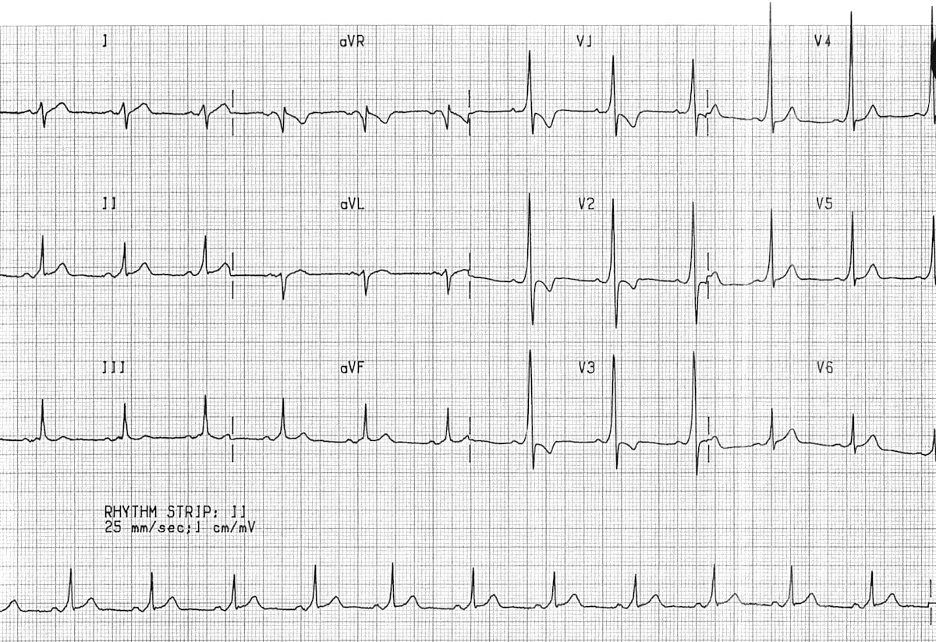
EKGs
- When interpreting EKGs, especially early on you need to be systematic
- A “significant” Q wave will be > 1/3rd the height of the R wave
- When you see STD, you should be asking yourself “where is the STE?”
- Most important factor to consider when evaluating for ischemia is the history, don’t get caught up too much on risk factors or lack thereof
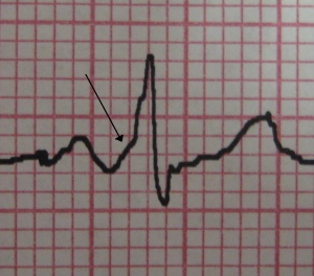
- Hyperacute T waves are broad-based, become asymmetric as the J point begins to elevate
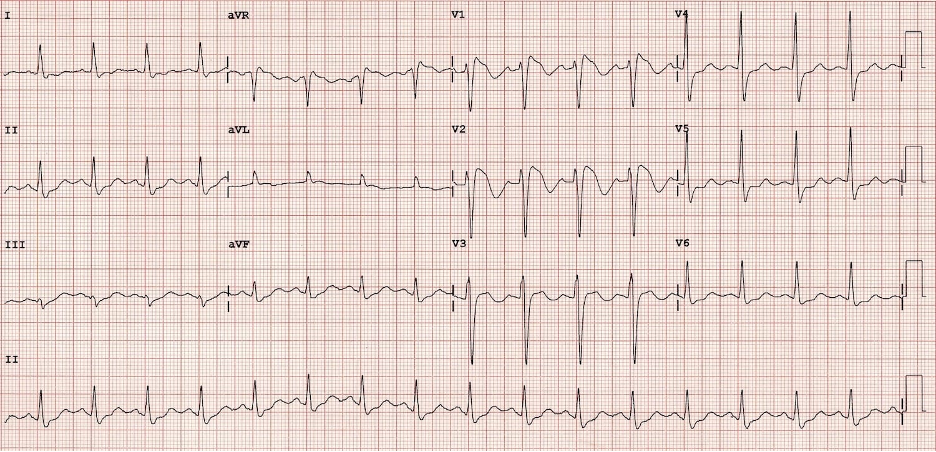
- Convex STE is very specific for ischemia
- Don’t forget to get serial EKGs when there’s any suspicion; If you’re repeating troponin, you should also repeat EKGs. Don’t be afraid to get a quick repeat in 15-20 minutes when they’re actively in chest pain and you’re concerned
R3 Procedure Sim: Pericardiocentesis + Transvenous Pacing
- Pericardiocentesis has three different approaches. No consensus on which is best
- If performing the parasternal approach be careful to avoid the thoracic artery
- Major indications for transvenous pacing include unstable bradycardia, sick sinus syndrome with pauses or failure to pace with the transcutaneous approach
- RIJ is the preferred approach for floating a transvenous pacer
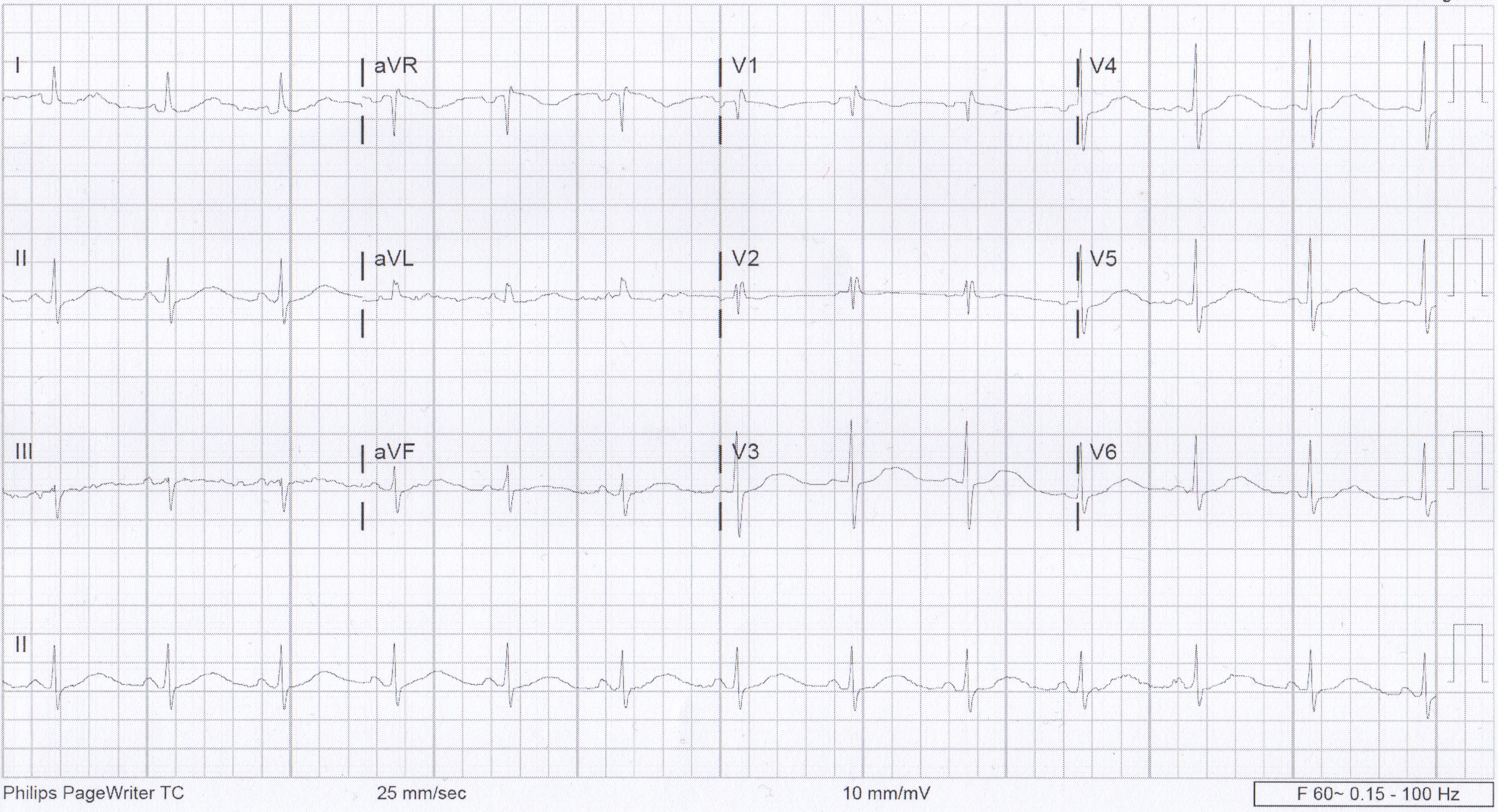
 We usually talk about QTc rather than just the QT. This is because the QT interval varies depending on the HR. Using a correction equation standardizes the interval so it can be interpreted regardless of the HR. The EKG computer does give a calculation of the QTc, because we are obviously not hand calculating this on every patient. You should compare what the computer calculates to your gestalt when you review the EKG. If there are any concerns or discrepancies, you should hand calculate the QTc.
We usually talk about QTc rather than just the QT. This is because the QT interval varies depending on the HR. Using a correction equation standardizes the interval so it can be interpreted regardless of the HR. The EKG computer does give a calculation of the QTc, because we are obviously not hand calculating this on every patient. You should compare what the computer calculates to your gestalt when you review the EKG. If there are any concerns or discrepancies, you should hand calculate the QTc.