![Room9er ["Room Niner"]:](https://room9er.com/wp-content/uploads/2020/03/cropped-Screen-Shot-2020-03-08-at-3.16.16-PM.png)
“Can you come see this patient in triage? Their knee is definitely dislocated.”
“Hey, doc, we’re bringing in this guy involved in an MVC, his knee was dislocated but it reduced on its own.”
It is important to be able to tell the difference between a true knee dislocation and a patellar dislocation.
Patellar Dislocation
A normally functioning patella is nestled within the trochlear groove of the distal femur. Patellar dislocations can occur either from a direct blow to the knee or from planting the ipsilateral foot and rapid change of direction/twisting, either of which can cause the patella to become displaced from the trochlear groove. Usually the patella becomes displaced laterally.


Reduction of the patellar dislocation involves extending the leg at the knee. Gentle pressure can be applied from the lateral aspect, directed medially, while extending. Post-reduction plainfilms should be obtained to evaluate for any associated fractures. If no fracture, the patient can be placed in a knee immobilizer for 7-10 days and follow up with orthopedics. Patellar dislocations are recurrent around 40% of the time.
Knee Dislocation
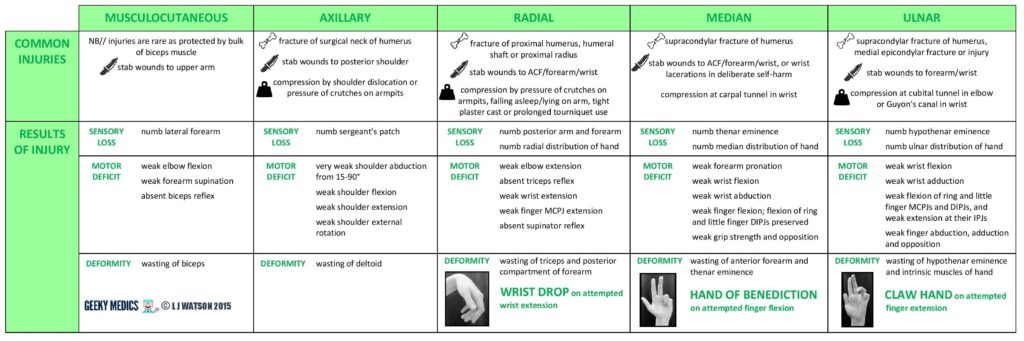
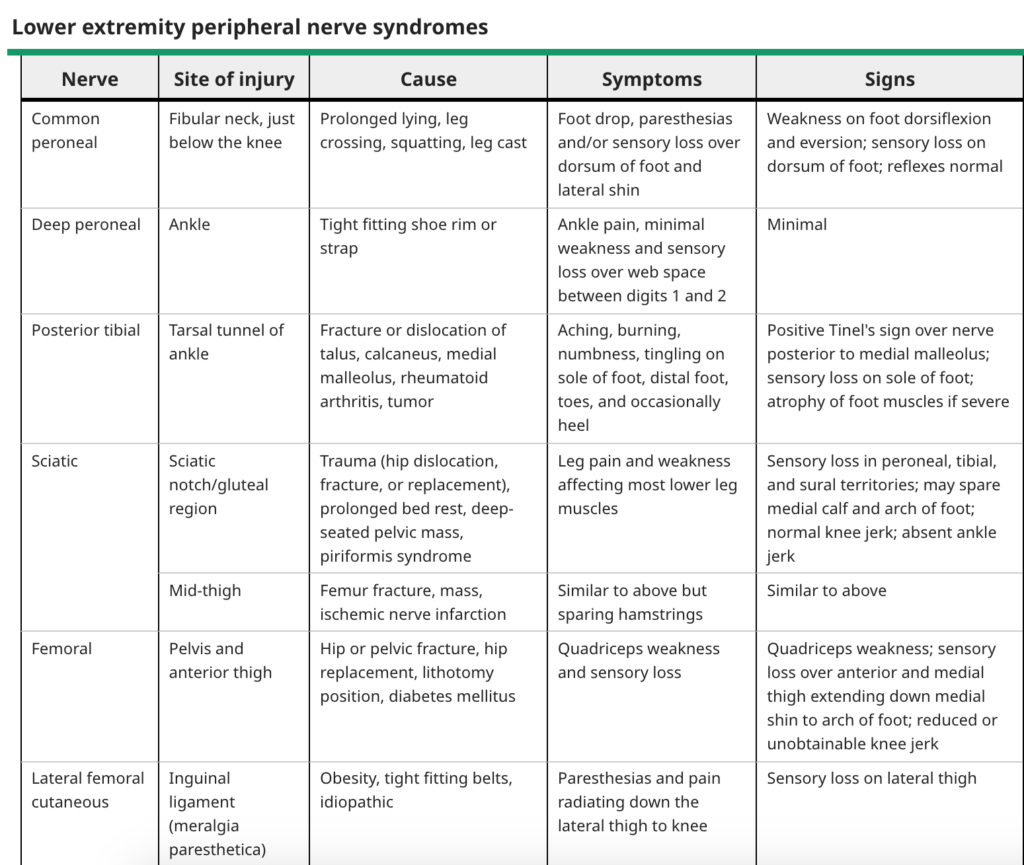
Knee dislocations are most commonly high mechanism injuries and have a high rate of neurovascular injury. They are rare, but it is difficult to know how many there truly are as up to 50% of them reduce spontaneously. The most common nerve injury is to the common peroneal nerve, with the popliteal artery being the most commonly affected artery. 60% of knee dislocations have associated fractures.

Treatment is emergent reduction and neurovascular examination. Presence of pulses does not exclude vascular injury. ABIs can be performed if pulses are normal. If ABI normal, may elect to observe the patient. If ABI abnormal, CTA indicated. If pulses are unequal, decreased or absent, you must ensure that the joint was reduced appropriately, and if still unable to locate pulses, immediate surgical intervention may be required.
Especially since both patellar dislocations and knee dislocations may spontaneously reduce, it is helpful to ask the patient and/or EMS about the initial appearance of the knee. A self-reduced patellar dislocation likely only requires plainfilms, while a self-reduced knee dislocation merits further evaluation for neurovascular injury.