Treatment = Stop offending medication, supportive care, Benzos
In TCA overdose, treatment for EKG changes is bicarb. Serial EKG’s to monitor following bicarb administration.
Dr. Lund- Peds ED
See sicker patients first
Lots of order sets for specific cases (neonatal fever, DKA, Asthma, etc.)
Vaccine status very important
Finish notes within 24 hours
All medical subspecialties aside from heme/onc admit to JFK (medicine)
Newborns eat 2oz every 2 hours on average
1 month oz, 4oz every 4 hours on average
Newborns may poop once a week or multiple times a day
Ibuprofen/Tylenol 10mg/kg every 6 hours, Ibuprofen > 3 months, Tylenol any age
Versed PO dose 1mg/kg, IV .1mg/kg, IN .2-.3mg/kg
Morphine .1mg/kg
Fentanyl 1mcg/kg
Need high dose amox to kill strep pneumo (pneumonia, AOM)
Bolus = 20cc/kg
Sepsis= 60cc/kg in first hour
Dr. Ferko- Shock
Shock = Hypoperfusion
Signs of shock – hypotension, tachycardia, decreased urine output, altered mental status
Types of shock- cardiogenic, obstructive, distributive, hypovolemic
Distributive shock- Example is sepsis. Inappropriate vasodilation.
Use lactic and blood pressure to determine severity of sepsis. Severe sepsis needs 30cc/kg bolus
Norepinephrine is first line. Vasopressin 2nd line. Then epinephrine or phenylephrine.
Cardiogenic shock- Most likely caused by acute MI. Severe decrease in cardiac output.
Norepinephrine is first line pressor again (pretty much first line for all shocks)
Distributive shock- Another example is distributive shock. Again, inappropriate vasodilation. Also classically involves no appropriate increase in cardiac output
Hypovolemic shock- In trauma, number one cause of shock. Treatment is blood or fluids, depending on cause of hypovolemia
Obstructive shock- Example is cardiac tamponade or tension pneumothorax. Decrease in cardiac output secondary to physical obstruction. Treatment is to relieve the obstruction.
Dr. Danzl- Law and Emergency Medicine
Document everything you do
When in doubt, treat the patient
Be kind and compassionate to your patients
Do everything you can to prevent patients leaving AMA. Give them the best chance to succeed if leaving AMA (give follow up, antibiotics as needed, etc.)
Take x-rays of all foreign bodies
Be sure patient can walk prior to discharge if they can normally walk
Always get a pregnancy test in women of childbearing age
What we don’t use anymore: Spotlight on ancient vomiting sticks!, Ipecac syrup (no longer in use 2/2 aspiration risk), EWOL tube (large bore gastric tube), Potassium permanganate
Activated Charcoal: binds drugs in a 10:1 ratio. The earlier the better (1-2 hours) and more efficacious with large, less polar molecules; dose 1-2g/kg (come in 50g tubes); CI with caustic ingestion, hydrocarbons, airway compromise, AMS
When to give multiple doses of AC
SDAC: single dose AC, used predominately for salicylates
MDAC: multiple doses AC, “gut dialysis” for drugs to undergo enterohepatic recirculation; single bolus dose (1g/kg) and then q8 hours (.5g/kg); do not use w/ sorbitol (diarrhoea); does not reduce M&M but does reduce drug rate
Carbamazepine
Lamictal
Colchicine
Dapsone
Phenytoin
Phenobarbital
Amatoxin
Quinine (hypothetical with hydroxychloroquine)
Whole Bowel Irrigation (1-2L Go Lytly 1-2 hours) best used for things not well absorbed by AC; packers (drug mules), XR preparations. Eg: Iron, Lithium, XR BB/CCB, bupropion. Note that this is a cumbersome and messy endeavour.
Gastric lavage: used with colchicine or paraquat (pesticide)
Take homes: AC best in the first 2 hours (but can argue to give beyond this), be familiar with MDAC, WBI for lithium and extended release substances
Workup: CBC, CMP, Blood (peripheral cultures are not routinely indicated)/urine cultures, CXR, LP if altered, Stool studies as needed based on symptoms
ALL: most common childhood malignancy; common presentation with fevers, lymphadenopathy, peteciae/purpura, hepatosplenomegaly, gingival hyperplasia, bone pain, hyperleukocytosis
Hyperleukocytosis: WCC>100k, high risk in infantile leukaemia, T cell ALL, AML, CML. Manage with hydration (#1) and consider alkalinised fluids without addition of K. Consider next adding Allopurinol and addition of Rasburicase (do not administer without consultation with haematology); avoid PRBC transfusion (increased risk of hyperviscosity)
Sickle Cell Anaemia: If pt presents with temp>35.5C, obtain CBC, blood/urine cultures, CXR, speak with haem/onc, antibiotics and admission of abnormal labs; can consider discharge if normal labs and OK with haem/onc/discussion with family/patient
Acute chest syndrome: SSA, plus chest pain, fever, SOA/hypoxia, new infiltrate on CXR. It is defined as a life-threatening lung infarction, common in 2-4 year olds, half of cases develop during hospitalisation and not at initial presentation. It is the second most common cause of hospitalisation in children with SSA.
Acute management: fluids, antibiotics, transfusion as needed (maintain hgb 9-11g/dL) for anaemia or severe hypoxaemia
Jonathan Boland, MD: Hernias
Reducible: soft, easy to replace; incarcerated: difficult to reduce, but retained blood flow; Strangulated: unable to be reduced, signs of ischaemia
Inguinal hernias are most common type of hernias; direct vs indirect
Femoral hernias: most common in women
Hernia management: if reducible> refer for outpatient management; if not reducible, CT and surgical consult. USS may be helpful but CT for definitive imaging
Tips for reduction, per Dr Eisenstat: pain control, Trendelenburg, ice hernia prior to reduction
Acalculous cholecystitis: high occurrence with systemic, life-threatening disease
Biliary Colic: recurrent attacks of upper abdominal pain, associated with evening hours, lasts no more than a few hours; caused by stone moving in and out of obstructing position. Treatment in the ER: pain control, outpatient surgery referral
Features of toxicity based on duration of ingestion
Acute ingestion: Rumack Nomogram, NAC therapy
Fulminant hepatic failure based on Cr, lactic acid, INR level
Mushroom toxicity
Amanita Phylloides
Eary vs Late onset (early onset suggest benign course)
Tx considerations: NAC, glucose monitoring, possible need for liver transplant
Shock liver: very ill patients, treatment is to treat underlying causes of shock
Jessica Javed, MD: Palliative Care/Hospice Elective Follow Up
Palliative Care: focused on symptom management, MDT, quality of life
Hospice: focused on patients who have less than 6 months to live, quality of life, pain management
Palliative care is available easily on an outpatient basis and can be arranged without admission
Hospice Takeaways: anyone can initiate a referral, inclusion criteria includes multiple ED visits for a chronic, unresolving medical issue, covered by most insurance, Hosparus is one of the only options for hospice in KY.
Tips for breaking bad news
Quiet setting
Create IDT with chaplain/nurses
Sit down if you can
Start by asking what the families know and fill in knowledge from there
Prepare family for bad news if appropriate
Give family/patient time to process
Tips for goals of care discussions
Focus on what the patient would want
Determine POA if patient is not decisional
Do give your recommendations
Don’t refer to full code as “doing everything”; this implies that everything else is not good/worthy
Goals of care can change; be open to this
Kentucky MOST form (Medical Orders for Scope of Treatment)
Makes goals of care more algorithmic
Usually used for hospice/palliative patients
Kept in the home
Can be used as a guide for caregivers/EMS (EMS must have original copy)/healthcare providers to direct what patient wants with regards to their care, especially in end of life situations
Generally reviewed annually or after d/c from healthcare facility
Dr. Dan Fisher and Dr. Mitchell Weeman did an awesome job with their clinical pathway summarising ER management of both upper and lower GI bleeds. See brief lecture summary below and find their clinical pathway uploaded to the site for a more in-depth review.
UGIB more common than LGIB; increased mortality with UGIB
GIB mimics: Pepto Bismol, Bismuth, Beets, red food colouring, bleeding from epistaxis/dental bleeding, red meat, iron supplements, vit C, horseradish, methylene blue
UGIB (proximal to ligament of Trietz; gastric>duodenal): most common aetioloy is PUD (NSAIDs, ETOH, ASA, Tobacco use), followed by erosive gastritis, oesophageal varices (high mortality) and Mallory Weiss tears; Risk stratification with Glasgow Blatchford Score
LGIB (distal to ligament of Treitz): most common aetiology haemorrhoids, diverticulosis/itis, aorto-enteric fistula (herald bleed), colitis, malignancy (ask about type B symptoms, Fhx), Meckels (in paediatric population)
ED workup: full history/physical, DRE, CBC, CMP (BUN:CR>36 w/o renal failure), type/screen, coags, guac stool test (if GIB can be pos for up to 2 weeks following), +/-lactic acid (risk stratification), +/- VBG (base deficit in acute setting), EKG (demand ischaemia), CT angio is test modality of choice for vascular cause of bleeding
Heparin à no renal metabolism (helpful in patients with renal failure)
Thrombocytopenia, HIT, heparin resistance, hyperkalemia from aldosterone suppression
Half-life 30-60 minutes, immediate onset
IV administration for VTE, must be administered inpatient
Careful monitoring required
Enoxaparin (Lovenox, LMWH)
Derived from heparin
3-5 hour onset, no monitoring required, patients may self-administer
Similar outcomes compared to heparin with regards to recurrent VTEs, some data suggest lower bleeding risk
Renal clearance, avoid in renal dysfunction
Similar precautions as heparin
Lower incidence of HIT, but still contraindicated in patients with HIT
Subcutaneous dose for VTE
Apixaban (Eliquis)
Factor Xa inhibitor
Half-life 9-14 hours, BID dosing
Renal clearance, caution in renal insufficiency
Rivaroxaban (Xarelto)
Factor Xa inhibitor
Half-life 5-19 hours, daily dosing
Must be taken with food to be effective
Renal clearance, caution in renal insufficiency
Dabigatran (Pradaxa)
Direct thrombin inhibitor
Half-life 12-14 hours
VTE dosing after 5 days of bridging, BID dosing
2020 AHS Guidelines on Management of VTE suggests using DOACs over Warfarin
Does not apply to all patients
AMPLIFY à Eliquis non-inferior to standard therapy (Warfarin, LMWH), less bleeding complications
EINSTEIN DVT/PE à Xarelto non-inferior to standard therapy
Does not recommend one DOAC vs. another, recommend using patient specific factors to guide clinical decision making
Recommends home treatment for patients with uncomplicated DVT
2020 AHS guidelines recommend considering home treatment for patients with low-risk PE (PESI Score risk stratification), conditional recommendation
Extremely important to counsel patients when being discharged on these high-risk medications, ensue follow-up and understanding of risks and return precautions
Pneumomediastinum (Dr. Alia)
Presence of free air in the mediastinum
Spontaneous (idiopathic, tobacco use, recreational drug use) vs. secondary (i.e. traumatic, iatrogenic) etiologies
30% have normal chest x-rays à CT Chest is preferred diagnostic modality
“Continuous diaphragm sign” on XR
Management:
Treat underlying cause
Supportive care à typically resolves spontaneously in 1-2 weeks
Disposition:
Primary à discharge with PCP follow-up
Secondary à management of underlying cause, typically will require admission
Lung Abscess, Parapneumonic Effusion, Empyema or (Dr. Edwards)
Typically polymicrobial, affected tissue at risk for necrosis and cavitation
Diagnosed via CXR vs. CT Chest (also recommended following XR diagnosis)
Ultrasound helpful for evaluation of effusions and for procedure guidance
Obtain blood and sputum cultures (blood cultures frequently negative in empyema)
Treatment à empiric antibiotics with anaerobic coverage
Empyema, effusions require drainage
VATS for complicated effusions and empyema
Thoracentesis provides definitive diagnosis for empyema (distinguishes between effusion and empyema) à body fluid cultures and diagnostics must be obtained
Pneumonia for EM Residents (Dr. Eisenstat)
CAP à everything not HAP or VAP
HAP à >48 hours from time of admission, previous admission within 90 days
Cover for pseudomonas and MRSA
VAP à >48 of intubation time, recent previous intubation
Cover for pseudomonas and MRSA
Therapy tailored based on sensitivities and culture results
Normal vital signs and normal respiratory examination have good negative predictive value in most patients
Procalcitonin à good predictor of blood culture positivity
Hypoglycemia, lactate à predictors of 28-30 day mortality
2-view chest XR recommended
Flu test patients with CAP during flu season
Give antibiotics to all patients clinically suspected to have CAP regardless of procalcitonin
Clinical judgement + decision tool is best (PSI > CURB-65)
Healthy, outpatient à amoxicillin vs. doxycycline vs. macrolide (if local resistance is <25%)
Comorbidities, outpatient à Augmentin vs. cephalosporin (cefpodoxime, cefuroxime) AND macrolide vs. doxycycline
Monotherapy with respiratory fluoroquinolone also acceptable, but consider risk factors
Inpatient treatment of CAP in adults without risk factors for MRSA or Pseudomonas
Combination therapy with Beta-lactam + macrolide or doxycycline
Coverage of anaerobic pathogens not necessary in admitted patients who are suspected to have aspiration PNA
Inpatient treatment of patients with risk factors for MRSA and Pseudomonas à vancomycin or linezolid for MRSA, Zosyn/cefepime/meropenem for Pseudomonas
Corticosteroids are unnecessary unless used in patients persistently hypotensive despite IVF and vasopressors (i.e. surviving sepsis guidelines) but evidence is not conclusive
Give Tamiflu to patients with CPA who test positive for flu (regardless of inpatient vs. outpatient or duration of symptoms), give antibiotics regardless of flu positivity
Antibiotic treatment duration for outpatient treatment of CAP à 5-7 days
No follow-up CXR necessary in adults who are improving following treatment
Assess hydration status (tears, saliva, capillary refill, wet diapers in 24 hours)
Check the ears (occasionally have coinfections)
Always do an abdominal examination to assess for hepatosplenomegaly
Management:
Suction! Suction! Suction!
CXR unnecessary unless concern for superinfection or clinical picture not consistent with typical bronchiolitis (prolonged symptoms, high fevers, persistent hypoxia) à atelectasis and peribronchial cuffing on CXR if obtained
Viral testing is not always necessary (exception: influenza, COVID-19, RSV <1 month causes apnea)
Respiratory support
Dexamethasone in patients <1yo with no history of wheezing did not demonstrate benefit
Albuterol has not been shown to benefit patients
Bronchiolitis Score is helpful with risk stratification
Discharge Criteria
O2 saturation >90% while awake
Adequate PO intake
Mild/moderate work of breathing
Reliable caretaker
Timely pediatrician follow-up in 1-2 days
Admission Criteria
Hypoxemia
Severe respiratory distress
Apnea
High-risk patients
Poor oral intake
Parents uncomfortable with discharge
Consider intubation if…
Recurrent apnea
Declining mental status
Not improving with respiratory support
Asthma Exacerbation
Antibody binds antigen à release of histamine/leukotrienes à inflammation à bronchospasm
Pediatric Respiratory Assessment Measure (PRAM) is helpful for risk stratification
Timing of medications is key!
CXR is not required unless concern for complicating factors
Management:
Beta-2 agonists
Albuterol à MDI vs. nebulizer
Always use a spacer!
Short vs. 1-hour long vs. continuous albuterol nebulizer
Discharge à take 4 puffs every 4 hours for the next 48 hours, then as needed after that
Remember to write for MDI with spacer if discharging with albuterol prescription
Terbutaline à IV vs. SQ
Corticosteroids à mainstay of treatment considering the pathophysiology
Dexamethasone
Prednisone/prednisolone
Methylprednisolone
Ipratropium nebulizer
Anticholinergic
Often used in conjunction with albuterol nebulizer
Magnesium sulfate
Smooth-muscle relaxer
Can cause smooth-muscle relaxation in the vasculature à hypotension (consider IVF bolus)
Epinephrine à anaphylaxis dosing
Admission Criteria
Requiring >1 1-hour long albuterol
Respiratory distress
Hypoxemia (O2 <92%)
Dehydration
Croup (laryngotracheobronchitis à upper airway)
Acute subglottic inflammation
Morbidity is greatest in 1st year of life due to narrower subglottic airway
Affects children aged 6-36 months
Classically caused by parainfluenza virus, but also caused by many other viruses
Clinical presentation:
Barky cough
Inspiratory stridor (more concerning if occurring at rest)
Tachypnea
Suprasternal retractions (hypoxia, intercostal retractions, abnormal breath sounds, subcostal retractions are uncommon à croup is a disease of the upper airway, if hypoxia is present and lungs are clear to auscultation there should be high concern for impending upper airway compromise)
Low-grade fever
Management
Dexamethasone
Racemic epinephrine for resting stridor or respiratory distress (can repeat every 15-20 minutes)
Monitor for 3-4 hours prior to discharge if administering racemic epinephrine à admit for refractory stridor or if repeat dosing of racemic epinephrine is required
Consider Heliox for severe respiratory distress as it decreases turbulent flow
Documentation Lecture (Ashley Chesman)
Critical Care Documentation
7.2% of all ED visits reported to Medicare in 2019 were reported as critical care
Time at bedside, but also time spent engaged in work directly related to the patient’s care:
Reviewing test results and imaging studies
Consulting services
Placing orders
Procedures billed separately
Billings starts at 30 minutes à critical care time requests <30 minutes may not be compensated
E/M and Critical Care Same Date of Service
Can now bill for E/M and Critical Care on the same date/visit
Documentation must support decompensation to a state requiring critical care
Remember to document critical care time beginning in residency!
Subclavian Central Venous Lines (Drs. Nichols and Leavitt)
Contraindications
Overlying infection
Anatomic obstruction
Fracture of ipsilateral clavicle
Relative à coagulopathy (harder to compress and apply pressure to the subclavian site)
Complications
Arterial injury
Pneumothorax
Air embolism
Cardiac dysrhythmia
Infection
Bleeding
Supra- vs. Infraclavicular Subclavian Access
Infraclavicular
Utilizes short-axis ultrasound
Index finger on the sternal notch and thumb at the midpoint of the clavicle at the angle
Make contact with the clavicle and “walk-down” and pass under the clavicle vs. insert needle further laterally to avoid having to “walk-down” the clavicle
Ultrasound assisted technique utilizes short-axis
Supraclavicular
Well-defined landmarks (claviculo-SCM angle)
1 cm superior and 1 cm lateral to the claviculo-SCM angle
5-15 degrees above the coronal plane
Don’t advance past 3 cm
Ultrasound assisted technique utilizes long-axis as opposed to the short-axes
Shorter distance from skin to vein
Larger target area
Straighter path to the SVC
Less proximity to the lung
Fewer complications compared to infraclavicular
Found to be non-inferior to the infraclavicular approach
Lightning Lectures – Pulmonary Cases (Drs. Bishop and Slaven)
Tuberculosis
TB concern à NAAT + sputum cultures to assist with diagnosis (95% sensitive)
Negative pressure room with airborne precautions, PPE precautions for providers, HIV test if TB suspected
Mycobacterium tuberculosis à aerobic rod, highly antigenic à can disseminate systemically if initial granuloma formation fails to contain the infection
Immunocompromised population at highest risk (2x)
bCG vaccine recipients all have positive TB skin tests (PPD)
Interferon test does not distinguish between latent and active TB
Active TB àINH, RIF, pyrizanimide, ethambutol x8 weeks à INH/RIF x18 weeks + B6
Hepatotoxicity
Latent TB à INH x9 months + B6
Must contact Public Health Department prior to discharge
Spontaneous Pneumothorax
Sudden pleuritic chest pain, increased work of breathing, hypoxia
DDx with examination + upright CXR
CT chest is very sensitive/specific but takes time to obtain
Consider US
Management:
Supplemental O2
Unstable à Decompression (treatment for tension PTX)
Stable, small à consider observation 4-6 hours, repeat CXR, must ensure follow-up within 24 hours à admit any recurrent or complicated PTX
Admit everything else and all PTX caused by comorbidities
Inhaled Intoxicants (Dr. Eisenstat)
Huffing/bagging à toluene is intoxicating substance (higher in gold and silver paints)
Can cause NAGMA, renal tubular acidosis, hypokalemia, chronic encephalopathy
Sudden sniffing death syndrome à hydrocarbon (huffing) + high levels of catecholamine surge à death
Generally not recommended to use epinephrine/norepinephrine in patients suspected of hydrocarbon toxicity
Aluminum encephalopathy from black tar heroin use à basal ganglia lesions on MRI
High water solubility à chlorine, tear gases, ammonia (mucous membrane effects)
Low water solubility à phosgene, chloramine, nitrogen dioxide (delayed pulmonary edema)
Phosphine gas/aluminum phosphide à occurs when aluminum phosphide interacts with moisture à can expose providers during ventilation efforts/resuscitation
Nitrogen dioxide à silo fillers
Phosgene à choking agent, delayed pulmonary edema
Tear gases à OC spray AKA pepper spray AKA mace à capsaicin-based tear gas à causes severe burning and irritation, CS (military grade) is more potent
Treatment is irritation (consider Morgan lens for eye involvement)
Organophosphates à nerve agents àdecontamination, atropine, pralidoxime, supportive care
Asphyxiants à methane, propane, argon gas à sudden collapse, helper also collapses, etc.
Carbon monoxide à can be high in smokers (COHgb of 10) and large cities
Treatment is controversial à begins with O2 therapy (100% FiO2, NRBM)
Consider hyperbaric in COHgb levels >25 (15 in pregnant patients due to fetal Hgb affinity for CO) or signs of organ dysfunction (AMS, NSTEMI)
The reason for HBO therapy is to reduce long-term symptoms, which are often delayed (up to 6-8 weeks), not life-saving
Cyanide à combustion of nitriles in house fires à leads to unconsciousness and CV collapse à elevated lactate (>8 with ingestion, >10 in house fires) with high suspicion
Amyl nitrite (induces methemoglobinemia) vs. Hydroxocobalamin/Cyanokit (safer, colors urine organe/red) with levels >8
Hydrogen sulfide à cellular asphyxiant similar to cyanide à rotten-egg smell in low concentrations (odorless in high concentrations), used in chemical suicide
COPD and Asthma Cases (Dr. French)
COPD à titrate goal O2 to 88-92%
Patients need PPV
Antibiotics for COPD exacerbation à some evidence for reduced rate of readmission/representation
Remember to consider breath-stacking/auto-PEEP in MV
PRAM Score for asthma exacerbation à follow-up 3 hours with additional PRAM Score, can assist with disposition planning
PRAM >12 à marker of impending respiratory failure
ED Management of Brain Aneurisms (Dr. Ding)
Unstable à repair
Stable à timely outpatient follow-up
1/3 will die, 1/3 will be self-sufficient at discharge, 1/3 will have poor recovery
Surgery (clip) vs. endovascular (coiling)
Treatment modality depends on multiple factors à age, medical comorbidities, multiple aneurisms, location, size, symptoms
Which aneurisms will rupture à location (anterior communicating, posterior communicating aa. higher risk) vs. size of aneurism vs. risk factors vs. family history vs. connective tissue disease/AAA vs. stress vs. growth of aneurism
Enlarging and symptomatic unruptured aneurisms should be treated
Before/after stent-coiling or flow diversion à DAPT
Consult NES for incidentally found aneurisms on imaging, both admitted and discharged
CTA/MRA for history of aneurism and symptoms
Consider SAH in post-coital headache
Don’t forget about LP vs. MRI in patients suspicious for SAH with negative CT/CTA
Interesting paper here, retrospective data pulled from the NEAR registry, a big high quality airway registry.
The take home point was NO difference in desaturations during induction in the ramp vs supine position. They reported DL and VL cohorts separately. Now I like to ramp patients, especially those with low GCS or obesity. So I am going to find the issues with the paper, and try to hold strong in my beliefs.
But seriously, there are some problems. It is retrospective. The patients who were ramped were probably sicker and more obese! It turns out they are:
However, obesity and subjective impression of difficult airway were more common in the ramped cohorts (Table 1) and independently associated with postinduction hypoxemia (Tables 3 and 4).
The paper is in AEM and therefore very well done. They perform adjusted analyses to try to tease out any real effects. But you cannot infer causation with this study. They do cite one paper on ICU intubations that found no benefit and possible adverse effects of ramping. But this study did not control for … wait for it … apneic oxygenation! Remember the post this week on airway success, apneic oxygenation is awesome, do it. But at least in this paper all patients had apneic O2.
Something else left out is how long they were ramped before intubation (i wouldn’t expect 30 seconds of ramping to help), they excluded trauma patients, they didn’t talk about how ramping can prevent vomiting / aspiration, they did mention that perioperative data suggests benefit to ramping : ).
Overall this paper is worth reading and the stats get pretty thick. Maybe a journal club in the future. But we have to be very careful making practice changes or any strong assertions based on a confounded (direct quote: “we are unable to control for unmeasured confounders”) retrospective paper.
Check out this paper in the upcoming Annals of EM. Data from the Videography in Pediatric Resuscitation (VIPER) Collaborative. Not a huge number of patients (494), but a solid N for a pediatric airway paper.
Research Pearl: Never just read the abstract, at least also look at the tables and figures! Then of course when you write a paper (or even an abstract), spend tons of time on your tables and figures, they are often the most efficient way to convey your findings to the reader.
Much of their findings are of course applicable to adult airway. Some interesting stats:
– The first-attempt success rate was 67%
– Median laryngoscopy duration 35 seconds (interquartile range 25 to 40)
– Hypoxemia occurred in 15% of the patients.
– Videolaryngoscopy was used for at least a part of the procedure in 48% of the attempts, and it had no association with success or the incidence of hypoxemia.
– Intubation attempts longer than 45 seconds had a greater incidence of hypoxemia (29% versus 6%). Furthermore, apneic oxygenation was used in 8% of the first attempts.
***What is happening? Why do we not set up apneic oxygenation on everyone? They had two of the 18 people (11%) with apneic O2 desat, but 18% of those with no apneic O2. Of course 18 is a tiny number and we can’t draw any conclusions, but there is no reason not to throw a nasal cannula (>15L) on every patient you intubate.
Take a look at Table 1 (pasted below), impressive intubation success for EM residents.
First-attempt success by provider category
Pediatric resident
1/1 (100%)
2/4 (50%)
3/12 (25%)
1/1 (100%)
EM resident
28/36 (79%)
7/9 (78%)
5/7 (71%)
7/10 (70%)
PEM fellow
61/112 (55%)
52/68 (76%)
12/20 (60%)
77/98 (79%)
PEM attending
7/11 (64%)
3/5 (60%)
0/3 (0%)
7/11 (64%)
PCCM fellow
13/15 (87%)
3/7 (43%)
NA
NA
Anesthesia
15/19 (78%)
17/22 (78%)
4/5 (80%)
7/9 (78%)
Other
NA
NA
NA
6/10 (60%)
Ok that’s probably enough for one post, check out the paper.
Acute unilateral facial paralysis with involvement of the forehead
Most common cause is idiopathic but there is association with HSV
Must exclude
Ear infection
Stroke
Forehead spared in central causes except if you have ipsilateral pontine pathology you can have forehead involvement and peripheral nerve presentation however will usually have CN VI involvement (check EOM)
Ramsay-Hunt syndrome from Herpes Zoster
Lyme disease (MCC bilateral Bell’s Palsy)
Tx
Steroids
Reduces relative risk of incomplete recovery at 6-12 mo
Prednisone 60-80 mg qd x 1 week
Ideal to start within 72 hours of Sx
Antivirals controversial
Supportive care if they cannot completely close their eye too keep eye moist and avoid corneal ulcers
Prognosis
15% can have permanent involvement
Follow up with ENT in 1 week
Trigeminal neuralgia
Paroxysms of severe unilateral pain lasting only seconds usually in the V2, V3 dermatome
80-90% caused by compression from aberrant loop of artery/vein
Can also be 2/2 MS, malignancy, AVM
Tx
IV phenytoin/Fosphenytoin
Abortive Tx lasts 4 hr – 72 hr
Carbamazepine
First line outpatient Tx
High risk of side effects
Posterior fossa microvascular decompression surgery successful in 70% of patients
Temporal arteritis, Dr. Boland
Temporal arteritis
Giant cell arteritis
Granulomatous, medium to large vessel vasculitis
Females 3x more likely
Rule of 50s
50 years of age, ESR > 50, treated with 50 mg prednisone daily
Cain cause painless ischemic optic neuropathy and blindness
Usually presents as a headache 85% of the time, can have jaw claudication, polymyalgia rheumatica seen in 50%, transient vision loss
Dx is confirmed by biopsy but if suspected start high dose corticosteroids prior to biopsy
If vision at any point during Hx loss admit, start IV steroids (methylpred), and have optho see
If no vision loss start high dose steroids (PO prednisone) and have optho see as soon as possible outpatient and biopsy between 1-2 weeks
ESR doesn’t have to be elevated (about 15% of time its not)
Pediatric endocrinology, Dr. Kopp
DKA
Considerations regarding fluid administration and cerebral edema in peds
PECARN DKA Fluid Trial
Compared fast and slow infusions of normal and half normal saline (4 arms)
Afterwards performed bedside evaluation of neurologic status (this is a clinical Dx not radiologic)
Bimodal distribution for presentation of cerebral edema
4 hours and 14 hours
3.5% had GCS decline <14, 0.9% had clinically apparent brain injuries
*Conclusion: neither the rate of administration nor the sodium chloride content of the IVF had contribution to the neurologic outcomes
Fluid replacement calculations
Fast replacement
Assume 10% weight-based fluid deficit, give the 20 cc/kg bolus isotonic IVF and replace the remaining with 2x maintenance over 24h
Dr. Kopp’s opinion: 0.45 NaCl given as a fast replacement strategy is preferred method as there was a higher incidence of hyperchloremic metabolic acidosis in the normal saline group (not statistically significant but study was perhaps underpowered)
Slow replacement
Assume 5% deficit give the 10 cc/kg bolus isotonic IVF and replace the remaining with 1.5 x maintenance over 48h
Dextrose containing fluids to be added when glucose is 200-300 (i.e. ~250) or when there is > 100 drop in glucose between 1hr POC glucose checks
Hypoglycemia
Rule of 50
Google and review it, V important
Consider inborn errors of metabolism in the differential of children who are hypoglycemic
Children with inborn errors of metabolism who present with acute illness, nausea, vomiting need prompt evaluation and immediate initiation of IV dextrose containing fluids and give them oral glucose immediately while IV access is being established. They can decompensate rapidly if kept in a catabolic state
Acute Coronary Syndrome or ACS is any condition that results in ischemia of the coronary arteries resulting in diminished perfusion of the myocardial tissue. There is a spectrum of cardiac diseases that fall into the designation of ACS including: ST-Elevation Myocardial Infarction (STEMI), non-STEMI (NSTEMI), and unstable angina. This discussion will center around STEMIs as well as introduce some STEMI-equivalents.
Chest pain is the most common presenting symptoms for ACS. However, 20-30% of patients presenting with ACS will present with atypical symptoms. There are associated risk factors for ACS as noted in the table below.
Atypical Chest Pain
Risk Factors for ACS
Dyspnea Nausea Abdominal Pain Dizziness Back Pain Palpitations
Age > 50-years-old Male Gender Tobacco Use Cardiac Family History Hypertension Diabetes Hyperlipidemia
Work-Up and Management
Patients presenting with concern for ACS should receive prompt electrocardiography (ECG) as well as CBC, chest radiograph, electrolytes, serum troponin, and PT/PTT. The 2013 American College of Cardiology (ACC) and American Heart Association (AHA) guidelines recommend serial ECGs in the first hour if there are concerning symptoms and the first ECG is non-diagnostic. The serial ECGs are important as approximately 15-20% of STEMIs are diagnosed on the repeat ECG. Missing a STEMI or myocardial infarction is one of the most common causes of malpractice for the emergency physician. The table below demonstrates the most common causes of losses in malpractice cases related to the cause of chest pain.
Most Common Causes of Malpractice Losses Related to Chest pain
Failure to obtain ECG Misinterpretation of ECG Failure to record data from clinical evaluation
Definition of a STEMI
Fourth Universal Definition of STEMI
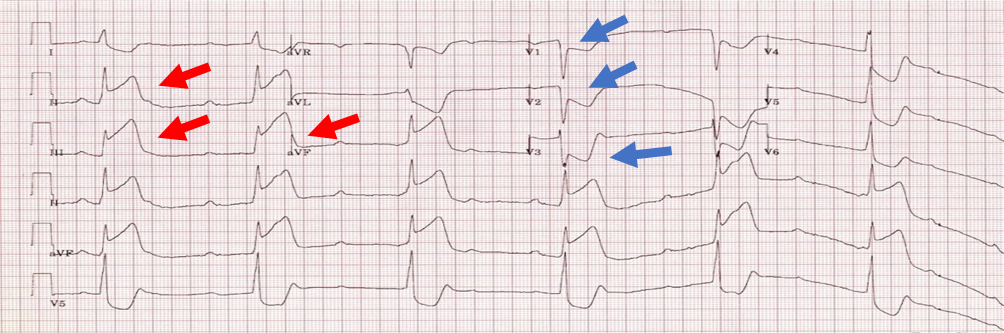
1 mm of ST elevation in any two contiguous leads except V2 and V3 In women: 1.5 mm elevation in V2 and V3 In men <40: 2.5 mm elevation in V2 and V3 In men 40 and older: 2mm elevation V2 and V3
ST-segment elevations are noted with the red arrows. Notice that there are ST-segment elevations in three contiguous leads: II, III, and AVF. There is usually reciprocal ST-segment depression in the opposite leads associated with ST-elevation myocardial infarctions. In this case of an Inferior Myocardial Infarction, there are reciprocal ST-segment depressions in the Septal and Lateral leads. This is denoted with blue arrows.
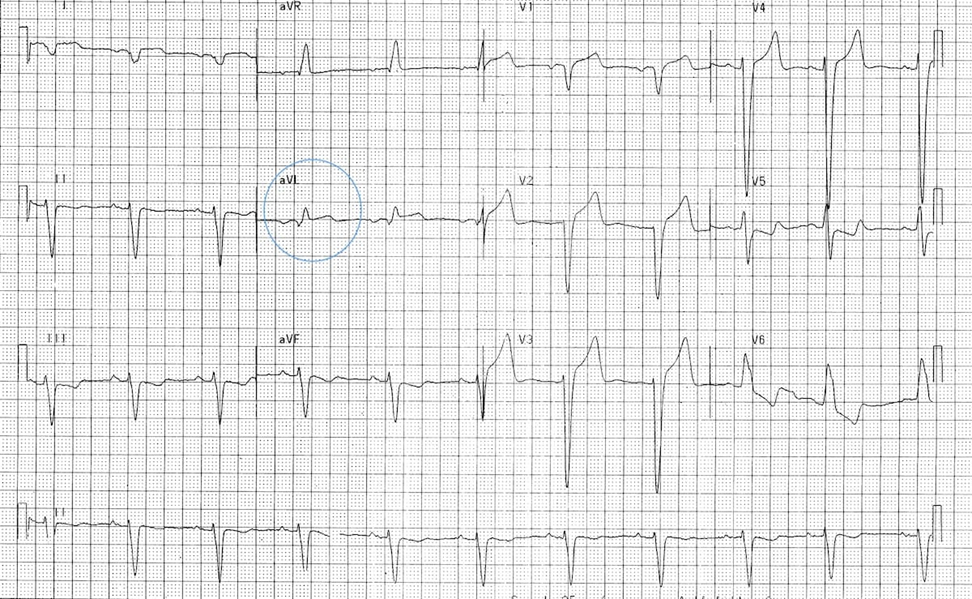
Wellens Syndrome
Wellens Syndrome refers to angina associated with T wave inversions in the left anterior descending coronary artery or LAD most notably in leads V2 and V3. Wellens Syndrome often presents in a pain-free state, but those patients who did not undergo reperfusion therapy with Wellens Syndrome noted on the ECG fared poorly with 75% developing an anterior wall myocardial infarction due to proximal LAD occlusion. Patients diagnosed with Wellens Syndrome should proceed urgently to cardiac catheterization.
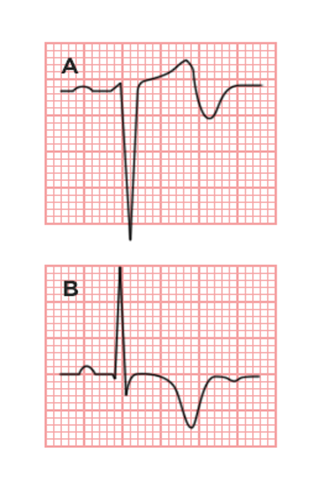
There are two types of Wellens Syndrome:
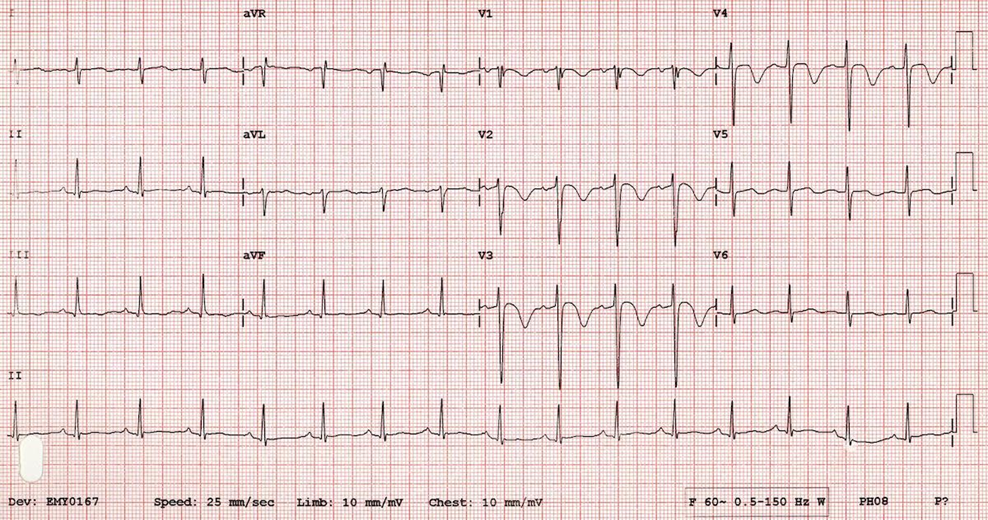
Type A is a biphasic T wave in V2 and V3 occurring in 25% of cases and Type B are deep, symmetrically inverted T-waves in V2 and V3 occurring in 75% of cases. (Picture from WikEM). In the EKG below from Life in the Fast Lane ECG Library , there are inverted T-waves in V2 and V3 consistent with Type B Wellens Syndrome.
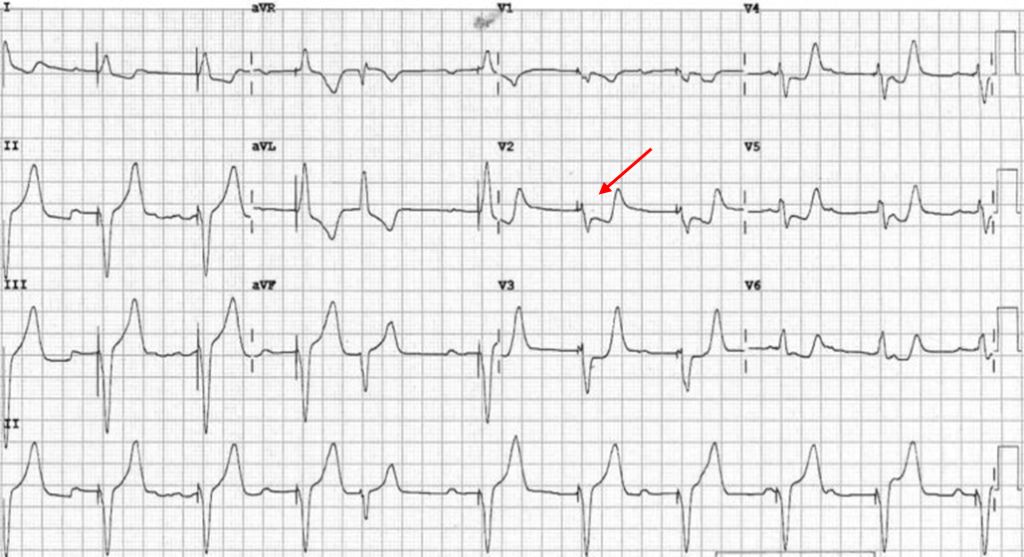
De Winter’s T Waves
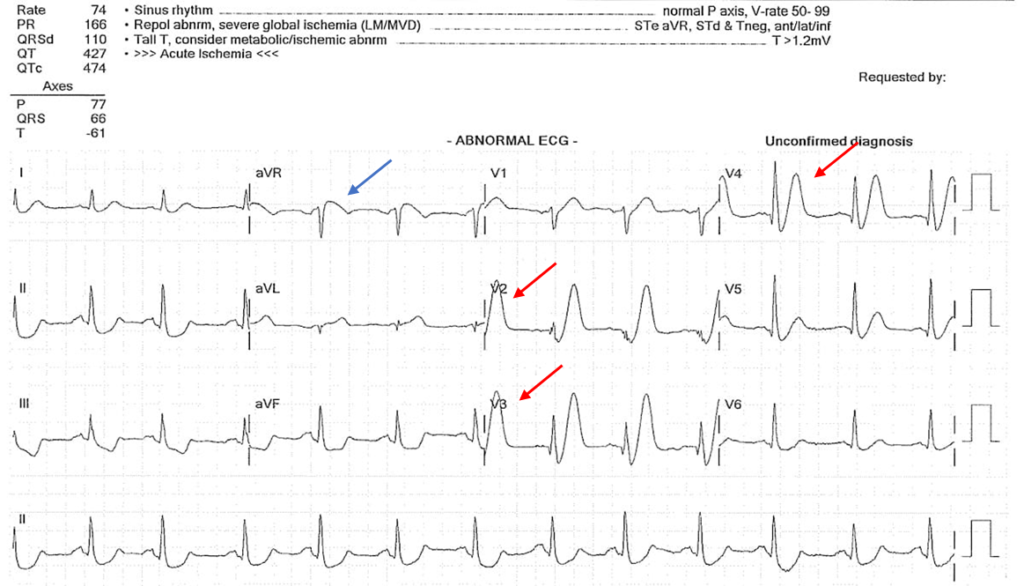
De Winter’s T waves were first identified in 2008 and account for 2% of proximal LAD occlusions making it a STEMI-equivalent requiring emergent cardiac catheterization. De Winter’s T waves are tall, peaked T waves in the precordial leads (V1-V6) with ST-segment depression at the J-point. In most cases, ST-segment elevation will be seen in lead aVR, however this is not specific.
In this figure, there are obvious peaked T waves in leads V2, V3, and V4 denoted by the red arrows indicating De Winter’s T waves. There is some ST-segment elevation in aVR consistent with this finding. A patient presenting to the emergency department with this ECG finding should go immediately to cardiac catheterization for likely LAD occlusion.
Left Bundle Branch Block with Myocardial Infarction
Previously, a new Left Bundle Branch Block (LBBB) was considered a STEMI-equivalent, however, recent literature suggests that a new LBBB does not often demonstrate increased risk of acute myocardial infarction. However, in 1996, Dr. Sgarbossa published a study of acute myocardial infarction in the presence of a LBBB with three criteria. Although the Sgarbossa criteria is not very sensitive, the findings were very specific for the finding of acute myocardial infarction.
Dr. Amal Mattu, professor of emergency medicine from the University of Maryland, separates the Sgarbossa criteria into three subsections: Category A, B, and C.
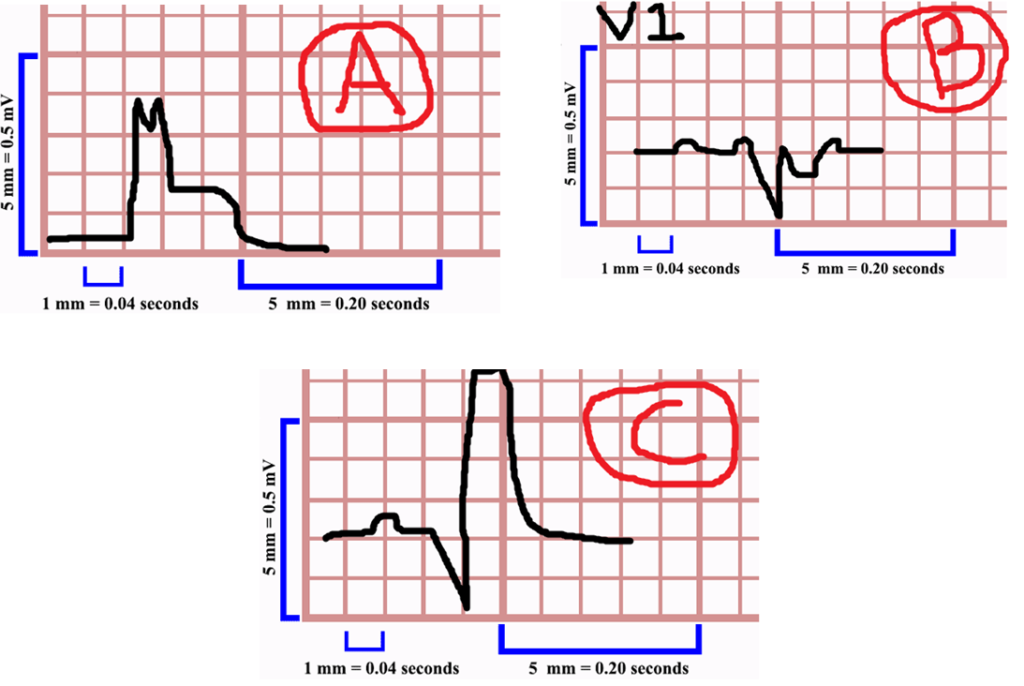
Sgarbossa Criteria
A. Concordant ST Elevation >1 mm in ANY lead B. Concordant ST Depression > 1 mm in V1, V2, OR V3 C. Discordant ST Elevation > 5 mm (not as specific)
In Sgarbossa A, the QRS complex is deflected in the positive direction (up) and ST-segment elevation is also present or concordance. If this occurs in any lead in the presence of a LBBB this is a STEMI-equivalent and the patient should proceed to cardiac catheterization. In Sgarbossa B, the QRS complex is deflected in the negative direction as well as the ST-Segment depression a shown in the example above in V1. If the ST segment is depressed in V1, V2, or V3 and the QRS complex is deflected downward this is also a STEMI-equivalent indicating acute myocardial infarction in the presence of a LBBB. Finally, in Sgarbossa C if the ST segment elevation is greater than 5 mm (or 5 blocks), this may indicate a STEMI-equivalent, however this is not as specific as criteria A or B. That being said, the finding of Sgarbossa C should prompt the physician to consult Interventional Cardiology as well as consider other signs and symptoms of ischemia.
Sgarbossa A:
Life in the Fast Lane https://litfl.com/sgarbossa-criteria-ecg-library/
In the above example, there is ST elevation concordance with the QRS in the presence of a LBBB in lead aVL indicating a myocardial infarction. Notice, that this is the only lead with ST-elevation >1 mm, but the criteria indicates that concordant ST-segment elevation in any lead with a LBBB is an indication for PCI.
Life in the Fast Lane https://litfl.com/sgarbossa-criteria-ecg-library/
In this example, there is concordant ST-depression in lead V2 in the presence of a LBBB indicating the need for emergent cardiac catherization.
Conclusion:
There are many findings on ECG that could indicate either a STEMI, STEMI-equivalent, or the presence of ischemia. It is important to note that there are a multitude of other ischemic rhythms and this is a brief and limited introduction to ischemic ECGs. Ischemia can be present even in the absence of ECG changes or changes in troponin, so history and physical still remain the most important methods in physician diagnosis of myocardial infarction and ischemia.
For further reading for acute care ECGs, I recommend:
Electrocardiography in Emergency Medicine by Amal Mattu, Jeffrey Tabas, and Robert Barish
ECGs for the Emergency Physician Volume 1 and Volume 2 by Amal Mattu and William Brady
Electrocardiography in Emergency, Acute, and Critical Care by Amal Mattu Jeffrey Tabas and William Brady
References:
AHA ACA – NSTEMI ACS Guidelines 2014
de Winter R, et al. A new ECG sign of proximal LAD occlusion. NEJM. 2008; 359:2071–2073.
de Zwaan C, Bär FW, Wellens HJ. Characteristic electrocardiographic pattern indicating a critical stenosis high in left anterior descending coronary artery in patients admitted because of impending myocardial infarction. Am Heart J. 1982;103(4 Pt 2):730-736.
Hennings JR and Fesmire FM. A new electrocardiographic criteria for emergent reperfusion therapy. Am J Emerg Med. 2012; 30(6):994–1000.
Lee TH, Goldman L. Evaluation of the patient with acute chest pain. N Engl J Med. 2000 Apr 20;342(16):1187-95.
Maloy KR, Bhat R, Davis J, et al. Sgarbossa Criteria are highly specific for acute myocardial infarction with pacemakers. West J Emerg Med. 2010;11(4):354-357. (Retrospective cohort; 57 patients)
Pope JH, Aufderheide TP, Ruthazer R, Woolard RH, Feldman JA, Beshansky JR, Griffith JL, Selker HP. Missed diagnoses of acute cardiac ischemia in the emergency department. N Engl J Med. 2000 Apr 20;342(16):1163-70.
Sgarbossa EB, Pinski SL, Barbagelata MD, et al. Electrocardiographic Diagnosis of Evolving Acute Myocardial Infarction in the Presence of Left Bundle-Branch Block. NEJM. 1996;334(8)
Thygesen, K et al. Fourth Universal Definition of Myocardial Infarction (2018). 2018 Nov 13;138(20):e618-e651.
Ünlüer EE et al. Red Flags in Electrocardiogram for Emergency Physicians: Remembering Wellens’ Syndrome and Upright T wave in V1. West J Emerg Med. 2012 May; 13(2): 160–162
As we know, point-of-care ultrasound has become an extremely useful tool in the ED, allowing providers to glean disposition-altering information from a quick and non-invasive bedside study. On my ultrasound month, I helped out with a patient who presented with shortness of air for 2-3 days. The patient was a fairly poor historian, but she reported progressive dyspnea on exertion for several weeks along with cough and orthopnea. She had no formal diagnosis of COPD or CHF, but she had an extensive smoking history. I was asked to perform a bedside echo to help narrow down the differentials. The images I obtained demonstrated some classic findings of right heart strain, and I felt like this would be a good opportunity to review some of them.
RV dilatation
Screen-Recording-2021-12-30-at-10.39.53-PM
As you can see in this parasternal long axis view from our patient, the RV is massively dilated in comparison to the LV. A normal RV : LV ratio is approximately 0.6:1. Anything larger than this is considered abnormal, with 0.6-0.9:1 representing mild enlargement, 1:1 moderate enlargement, and > 1:1 severe enlargement. When looking at the parasternal long axis view, you can use the “rule of thirds”. According to this, the left atrium, LV outflow tract, and RV outflow tract should be roughly the same size. In this video, the RVOT is clearly much larger than it should be. You can also get a sense of the relative sizes of the ventricles in the other three windows on transthoracic echo.
RV systolic dysfunction
In our patient’s apical four chamber view, you can again appreciate the size of the RV compared to the LV. In addition, there appears to be relative hypokinesis of the free wall of the RV, suggesting there is systolic dysfunction. The right atrium enlargement seen in this video also suggests that this patient’s RV strain was more of a chronic process.
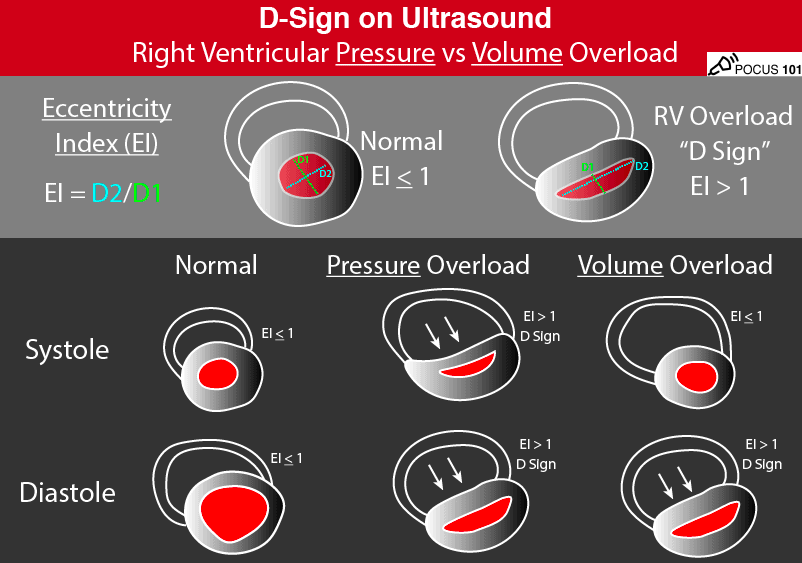
Paradoxical septal wall motion
In a normal heart, the LV should be fairly circular in the parasternal short axis view, and the RV will appear more crescent-shaped. Additionally, the walls surrounding the LV should move inward equally during systole. In the setting of elevated RV pressures, you can often see the interventricular septum bowing in towards the LV, creating a “D” shaped left ventricle, as seen in the clip above. Interestingly, there are different variants of the so-called “D sign”, helping to distinguish between right ventricular pressure vs. volume overload. In pressure overload, the RV presses on the septum during systole AND diastole. Conversely, in volume overload, the septal bowing is much more pronounced in diastole compared to systole. Our patient has a D-shaped LV throughout the cardiac cycle, suggesting RV pressure overload.
McConnell’s Sign
This finding refers to RV wall hypokinesis with apical sparing. As you can see in the video above, the apex of the RV appears to bounce up and down while the rest of the RV remains stationary. In the right clinical setting, McConnell’s sign is considered highly specific for acute pulmonary embolism. Disclaimer:this clip came from one of Dr. Nichols’s patients who was later found to have an extensive saddle embolus.
Lack of respiratory variation in the inferior vena cava
The normal IVC diameter is less than 1.7 cm and there is a 50% decrease in the diameter during inspiration when the RA pressure is normal (0-5 mmHg). When the inspiratory collapse is less than 50%, the RA pressure is usually between 10-15 mmHg. If there is no collapse with respirations in a spontaneously breathing patient, this suggests markedly increased RA pressure > 15 mmHg. This is usually best evaluated using M mode, measuring the diameter of the IVC during inspiration and comparing to its diameter during expiration. Our patient has an enlarged IVC with almost no collapsibility throughout the respiratory cycle.
Conclusion
If you identify any of these findings on a patient in the emergency department, you should consider common causes of RV failure and strain, such as PE, pulmonary hypertension, left heart failure, ARDS, severe tricuspid regurgitation, volume overload, etc. Our patient received a CT PE in the ED, which was negative. She was subsequently admitted to the cardiology service, where right heart catheterization found evidence of severe pre-capillary pulmonary hypertension. After a few days of monitoring, she was subsequently discharged back into the world with a prescription for diuretics and follow up in the pulmonary clinic.
Highest mortality rate due to proximity to mediastinal structures
Zone 2: Cricoid cartilage to angle of mandible
Most commonly injured
Classically, zone II injuries undergo surgical exploration, zone I and III undergo further evaluation
Zone 3: angle of mandible to base of skull
Penetrating trauma:
Has to penetrate the platysma which demarcates superficial from deep wounds
Most common cause of immediate death is involvement of carotid artery
Hard signs of vascular injury:
Hypotension
Arterial bleeding
Rapidly expanding hematoma
Deficits (pulse/neuro)
(bruit/thrill)
Hard signs of aerodigestive trauma:
Air bubbling, massive hemoptysis, respiratory distress
Soft signs
subQ air
dysphonia
dysphagia
Blunt Trauma
Blunt vascular injury have up to 60% risk of stroke; if no operative intervention, consider ASA/Plavix/heparin etc
Denver Screening Criteria
Used to screen for vertebral and carotid artery dissection and/or injury after blunt head/neck trauma
CTA if 1 or more criteria present
Reduces number of missed injuries to <5%
Strangulation
Most common cause of death is neck vessel occlusion rather than airway obstruction
Also can have laryngotracheal fx, C-spine injury
If dyspnea, dysphonia, odynophagia, etc need laryngobronchoscopy
Ophthalmic Trauma Dr. Nelson
Corneal abrasions:
Richly innervated = very painful
Short healing time 24-48 hours
Common causes: mechanical trauma, foreign body, contact lenses, flash burns
Clinical features: foreign body/gritty sensation, injection, tearing, relief with topical anesthetic, can also have photophobia and vision change
Workup and diagnosis: eyelid exam with eversion, fluorescein exam looking for uptake
Consider corneal ulceration in contact lens wearers
Treatment: Removal of foreign body, PO/topical NSAIDs, abx (erythromycin in general population, fluoroquinolone drops in contact wearers for pseudomonal coverage)
AVOID pressure on the eye = do NOT perform tonometry
May have positive Seidel’s test on fluorescein exam
CT orbit if concern for foreign body
Management: urgent ophtho consult for repair, cover eye, elevate HOB, bed rest, tdap, abx
If no foreign body, IV fluoroquinolone
If foreign body, IV vanc+ceftaz
Eyelid Lacerations:
Ophtho consult for repair:
Lid margin
Within 6-8mm of medial canthus
Lacrimal duct/sac
Inner surface of lid
If ptosis is present
Tarsal plate or levator palpebrae involvement
Full thickness (through and through): high risk for ocular injury, eval for corneal lacs and globe rupture
Partial thickness: most simple horizontal lacs can be repaired by ED physician, ends of sutures should be kept away from cornea to prevent further abrasion
Lid margin lacerations: very small <1mm do not need repair and will heal spontaneously, if larger consult ophtho for repair
PEM Lecture-Abdominal Trauma: Dr. Elmore
Trauma is the most common cause of death in children from 1-18 years old in the US
Blunt abd trauma accounts for more than 90% of childhood injuries
It is the most unrecognized cause of fatal injuries
Children are at greater risk due to immature skeleton and they have higher abd organ to body mass ratio
Children are able to compensate in the face of significant blood loss
Clinical prediction rule may rule out intraabdominal injury in blunt trauma
No sign of abd wall injury
No TTP
No evidence thoracic wall trauma
No abdominal pain
No decrased bowel sounds
No vomiting
HDS but concern for intraabdominal injury if:
Hct<30
UA>5 RBCs
AST>200,ALT>125
Elevated lipase
Low systolic BP
Femur fx
Spleen most commonly injured intraabdominal organ, liver second
Pancreatic injury = classic “handlebar” injury from bike accident (also consider duodenal injury/hematoma with this mechanism)
Hollow viscera injuries are rare, but most common causes are lap belt injuries, peds vs. auto, NAT (rapid acceleration/deceleration)
As many as 50% of children with Chance fx have intra-abdominal injury such as duo perf, mesenteric disruption, transection of small bowel, panc injury, bladder rupture
TEN-4 rule for NAT
Bruising on torso, ears, or neck of child >4 years old
Any bruising in an infant 4 months old or less
Small Group: Abdominal Trauma Dr. Harmon
Indications for immediate lap in penetrating abdominal trauma:
![Room9er ["Room Niner"]:](https://room9er.com/wp-content/uploads/2020/03/cropped-Screen-Shot-2020-03-08-at-3.16.16-PM.png)