Everyone should view this NEJM video on examination of the shoulder.
Cold Shoulder
Reply
![Room9er ["Room Niner"]:](https://room9er.com/wp-content/uploads/2020/03/cropped-Screen-Shot-2020-03-08-at-3.16.16-PM.png)
Everyone should view this NEJM video on examination of the shoulder.
The how to stay healthy in EM posts on Aliem are definitely worth checking out. One common piece of advice given on tolerating the night shift is hydration. Here is a cool study proving this, many studies like this in the literature.
Bosse’s favorite molecule (and lab test), lactate has a sordid and confusing history. This article in Emergency Medicine News sheds some light on lactate and its role in disease (or health). The author (Dr Paul Marik) is board certified in internal medicine, critical care, neuro-critical care and nutrition.
It may take a couple reads but this article has a succinct, common sense approach to understanding lactate production and use by the body. You may not be able to apply this knowledge on your next patient encounter, but physiology is fun right?
I will apologize for the wall of text in advance but I thought I to share an experience from last May that fits pretty well with the first 2 weeks of lectures this month. I think it definitely highlights the importance of feeling comfortable with both delivery and newborn resuscitation in case they actually happen to you. I’ve also tried to point out all problems that came about but I am sure I didn’t hit them all and I am positive that I could have handled some of them better.
It was nearly the end of a pretty typical shift at Jewish Downtown. For those of you who haven’t been there or don’t know there is zero OB coverage at Jewish. I was finishing my charts when I hear the secretary say “pregnant woman in labor” over the phone. That is a pretty unusual thing to hear at Jewish so I immediately asked the attending who was sitting closer if I heard that correctly. I also half-jokingly said I definitely wanted in on the patient if they were serious because I still needed a few more deliveries. The attending chuckles and replied that she thought the secretary was only joking because there shouldn’t be any reason for a laboring patient to come to Jewish, so I returned to my charts.
About 2 minutes later they call for a physician from the room behind the doctors area and we walk into what is in fact a laboring patient. The nurses state she seems to be contracting every 3-4 minutes but they don’t know much else at this point. While the attending checks her cervix, I grab the ultrasound and check the fetal position. She was about 8cm dilated and the best I could tell the baby was vertex but the head was so far down I gather this from the rest of the anatomy. Immediately calls start going out to the neonatologist at Kosair while we attempt to talk to the family and figure out how the patient ended up at Jewish. Here comes out first problem:
Problem 1: Neither the patient nor the family speak a word of english. Not only that but there is no translator phone in the room so the family has to be taken to another room to try to get some questions answered.
In the meantime I attempt to get a fetal heart rate to assess how the fetus is doing.
Problem 2: The only doppler is a pen style for checking pulses that doesn’t actually display a pulse number.
I go back to the ultrasound, find the heart and count the beats on the screen while a nurse counts for 15 seconds to get a FHR of about 144, which is always reassuring. In the mean time we are able to obtain some more information from the family.
Apparently, the patient’s water broke during her office visit around 2pm (it’s now almost 11pm) and she was told to go to the hospital. For whatever reason they decided to wait and they got mixed up between Norton’s and Jewish hence our current situation. There are calls being made to Norton’s L&D informing them of the situation and transport is on the way. The neonatologist is also en route as a safety precaution in case she actually delivers here. The patient and fetus appear to be stable, and while still contracting around every 3-4 minutes she still isn’t fully dilated. I make the mistake of leaving the room assuming that the patient will soon be swept away to have her baby properly on an L&D floor. About 5 minutes later another call from the room and I walk in to see the beginning of this baby crowning.
The nurses wheel in their delivery kit as I gown and glove up. I apply a few packets of lubricant jelly, have the nurses move the patient closer to the end of the bed and attempt to create a semi-sterile field with the supplies available.
Problem 3: It’s nice and easy to set up to deliver in a room with a bed designed to deliver a baby. Unfortunately for me this situation involved a nurse/tech on each leg and the patient mostly laying flat in a bed with bag to collect fluid half hanging off the table but mostly just shoved under her bottom as best as I can with no real drainage.
Problems 4 & 5: Did I mention she didn’t speak english, also I have no idea what the word for “push” is in her language. Also when you are on the L&D floor you have all kinds of cool toys such a tocometer to help you know when to tell the patient to push. I do not have that luxury.
I attempt to put a hand on her abdomen to feel her uterus contract so I know when to tell her to push and hope that she figures out what we want from her. Maybe it was a good thought but I have no idea, good thing she does and she is pushing every few minutes and the head is progressing it’s way out.. After a few good pushes the progress seems to slow a little bit and I start to worry a little bit that this 2 week post-dates baby may be stuck. What was that mnemonic for shoulder dystocia again? All I can remember is McRobert’s maneuver, but for anyone curious, Rosen’s has a nice one:
Help: Obstetrics, neonatology, anesthesia
Episiotomy: Generous, possibly even episioproctotomy
Legs flexed: McRoberts’ maneuver
Pressure Suprapubic pressure: shoulder pressure
Enter the vagina: Rubin’s maneuver or Wood’s maneuver
Remove posterior arm Splint, sweep, grasp, and pull to extension
Luckily, I have the nurses holding onto each leg (because this bed doesn’t have stirrups) so they flex her legs towards her as much as they can and everything continues to progress smoothly. Eventually the head is out and the rest of this baby boy delivers quickly. He is suctioned, wrapped in a warm blanket and the nurses begin assessing him. I think we put his APGAR at a 7 at 1 minute.
So I am done right? Baby is out, nothing more to see or do, lets ship them out. Right?……
Turning back to the patient I realize she seems still be bleeding a little more than I expected. It’s hard to figure out where she is bleeding from so I deliver the placenta which appears to be intact. I even sweep and massage the uterus just to be sure which seems to be contracting well.
Problem 6(?): Not really a problem because it seems her bleeding was not coming from the uterus but I have no access to the medications typically used to help control uterine bleeding after a deliver such a pitocin. Not that it matters because I didn’t know what the dose would be anyway. Just another interesting thought that I had during this whole process.
Since the placenta is whole, and seems to be firm I look for other sources of bleeding. This is when I realize the patient has a nice 2nd or 3rd degree tear (Dr Sterrett would be very disappointed I didn’t control the head well enough). I check to make sure it isn’t a 4th (thankfully it’s not), and start contemplating my next course of action. The attending asks what kind of suture I want to use to repair her tear. My only reaction was to smile and say “nothing”, followed by explaining that since the bleeding is slowing it’d probably be better to let the OB-GYNs fix her. I plan to pack her to make sure she doesn’t bleed too much in transport.
Problem 7: No one had even seen a vaginal packing kit in the ED before, so we improvised and used some kerlex with a tail for easy removal.
By the time this had finished the neonatologist had arrived and began assessing the newborn. I think we ended up giving him apgars of 7 and 9. I started the patient on some fluids (because we didn’t have an IV when all of this started, another mistake I didn’t realize until it was all over) and within another 2 minutes transport had arrived to take the patient to Norton’s and she was actually swept away. Hopefully the OBs she finally got to didn’t think I botch the whole thing too much. Overall it was a pretty intimidating and adrenaline pumping situation. Not sure if I will ever have an experience quite like this again but if it does happen at least it will not be the first.
Any comments, critiques, criticism or otherwise are welcome.
Just this month, the UL ID department presented lectures on research methods from the beginning to the end of the research process.
Louisville Lectures has posted the first 3 of them and they are fantastic as expected. Louisvillelectures.org continues to receive praise from Lifeinthefastlane blog. You can find the lectures on Youtube or iTunes as well.
Here is a link directly to the site, they are video lectures so I would recommend watching on this link, though if you like to listen while driving check podcasts on iTunes.
The lectures are brief enough to be valuable for all residents and faculty, worth repeated views for anyone interested in academics.
Flumazenil (Rx: Romazicon) has recently been described as coming into favor for two unique purposes: (1) hepatic encephalopathy and (2) paradoxical reactions to benzodiazepines.
Regarding the first, flumazenil’s use in hepatic encephalopathy has been well described recently in a Cochrane review of 113 RCTs with a total n = 805, wherein flumazenil had a significant beneficial effect on short term improvement of hepatic encephalopathy.1 This is thought to occur physiologically secondary to reversal of the origin of hepatic encephalopathy—i.e., an accumulation of substances that bind to a receptor-complex in the brain resulting in neural inhibition1 (principally GABA receptors which are forefront in the stimulation of sedation). Therefore GABA receptor antagonists (such as flumazenil) can be used to directly oppose this mechanism. Effect on full recovery and survival has still not been proven with flumazenil administration.1
Secondly, flumazenil can be used for paradoxical reactions to benzodiazepines2,4 and in a 10 year review of its use, published in the Journal of Emergency Medicine,3 the real safety of this drug has once again come into question, as there were relatively few adverse outcomes even in the highest of seizure provocation risk—which occurred with co administration of pro-convulsant (e.g., TCAs) at a 2.7 % incidence (8/293)—the total incidence including all subjects bore a rate of 1.4% of seizure activity (n = 904).3
I present an example of administration in the second of indications above. I took care of a 26 yo WF with PMH of asthma, a prior severe dental cavity pending root canal and an IV heroin addiction, currently sober and progressing through the the 12 Steps program at the Healing Place. She presented in sepsis, afebrile with qSOFA of 0/3 (Labs: WBC 21.2 with left shift, procal 1.33, ESR 83, CRP 201, lactic acid 0.8 s/p 2 L NS IVFs), and AKI (Cr. 1.6) with dental as well as urinary possible sources. She was eventually discharged on day 3 with Dx of urosepsis, creatinine returned to normal, and had a negative echo for routine endocarditis rule out in the setting of PMH of IVDA.
During her ER stay she was uncomfortable, diaphoretic, pale, GCS of 15, but anxious and in pain, professing severe insomnia for 3 days, stating, “I just want to sleep”. A trial of oral Ativan 2 mg was given, as she did not want any pain medication due to her prior addiction. She noted a small temporary improvement; however 2 hours later this beneficial effect was absent. By now she had received cefepime 2g and vancomycin 25 mg/kg (for potential osteomyelitis coverage), and was requesting more anxiety medications, having already received 50 mg IV Benadryl 30 minutes prior with no improvement noted. Clinically she was GCS 15, pleasant in interaction, increasingly pale, uncomfortable, wide awake at 0445, and subjectively in pain. She was then given 2 mg IV Versed.
Immediately following the administration of midazolam she became altered to GCS 12 (E4, V3, M5), eyes wide, extremities tremulous, pulled out all of her IVs, and was trying to jump off the bed. It was clear she was paradoxically agitated and hyper-aroused. Rather than reversing her (though we doubted history of benzodiazepine use), we opted to watch and see if this reaction would subside without intervention since she responded favorably to the oral Ativan; however the rarely seen but well known paradoxical reaction to Versed was suspected. She was observed 1:1 and thereafter 3:1 for 40 minutes, at which time she appeared to be steadily worsening rather than improving. The decision was made to give an IV push of 0.2 mg of flumazenil (Rx: Romazicon). Within 30 seconds after administration she once again returned to her pleasant self, she was GCS 15, appropriate, and had no recollection of the previous hour, and had no seizure activity noted throughout her stay. She maintained a healthy mental status of GCS 15 and was AAOx4 for the rest of her evaluation and admission.
In 2010, Kreshak et al. reported a similar case and treatment. This paradoxical reaction to Versed in their report is thought to occur at less than 1% incidence, however it is described as commonly as 1.4 %.4 In the reported literature this reaction is described as a patient becoming acutely agitated, restless and aggressive2. Stiffening and jerking of the extremities, and shaking of a part of the body are also noted. When observing a patient with this reaction, after ruling out other etiologies of agitated AMS, Kreshak et al. (2010) opted to administer flumazenil 0.5mg IV, and “…immediately after which the patient became conscious, oriented and calm, the paradoxical reaction was terminated”. The patient had no recollection of the events,2 similar to the patient observed in the ULED.
Per Kreshak et al. (2010), there exist “…different theories concerning the mechanism of paradoxical reactions, involving a central cholinergic effect or the serotonin imbalance”.2 Unfortunately the exact mechanism of paradoxical reactions remains unclear.
Although difficult to locate literature, if seizures develop following flumazenil administration, pharmacology guidelines recommend Valium 20-30 mg IV then immediately switching to barbiturates; some soft EM sources also suggest going straight to propofol.5
Thank you for reading my post.
References
Case: 57 yo M who presents via EMS found with circumferential burns on bilateral lower extremities, left upper extremity, lower pelvis, and left side of chest after being trapped in a burning tent. Unknown time of incident.
VS: HR: 128, RR: 24, BP: 112/64, SpO2 96% on 4L O2
Alert, oriented x 2. SEVERELY DISTRESSED. Singed nares bilaterally. Bilateral wheezes, tachypneic. Tachycardic, RR. Abd S/NT/ND. Once again, 3rd degree burns circumferential burns from lower pelvis, extending to groin, and down to bilateral lower extremities. The 3rd degree burn covered the left side of his chest and his RUE. No pulses were palpated in his LUE or BLE. Though burned, BLE and RUE appeared blanched with poor cap refill and cool to touch. 72% estimated burn coverage total. Pt stated he was unable to feel or move bilateral lower extremities.
During the process of IV, O2, monitor, and moving the pt over. I called for pain medication, intubation meds, and got the equipment ready for intubation.
Trauma, Plastics, Urology – paged. Don’t wait to get consults on board in a case where you are preparing to do this procedure.
On physical exam, remember Wallace rule of nines (see total body surface area): 9% for each arm, 18% for each leg, 18% for the front of the torso, 18% for the back of the torso, and 9% for the head and 1% for the perineum. At the same time, think Lactated Ringers at 4 mL x kg x percentage burn = total fluids needed for replacement in initial 24hrs. First half of amount in first 8 hours with the second half over 16hrs{{Parkland}}.
But, first, intubate to secure the airway, provide pain control, and facilitate further exam. Needless to say, burns are extremely painful.. . so are escharotomies.
Trauma wedge took the RLE, and I had the LLE. In the race to get pulses back, I succeeded and was rewarded with getting to do the LUE as well.
How did I perform the procedure you ask? Well, it was with the Trauma fellow standing at the foot of the bed giving instructions and guidance . .. I had never seen anything like this except for textbook cases of a circumferential burn to the chest/trunk. This procedure is not on our sign off list, required list, or on anything that I had seen in cadaver lab.
While these procedures are as rare as a Trauma fellow eager to teach at 2 am, you may be faced with the same in a rural ED or with a wedge stuck in the OR, etc.
Advice: Be nice to your colleagues. And, more importantly, prepare.
Here are some very informative links that would’ve been great to have seen or reviewed prior.
Video 2: Australian Escharotomy How-to
FYI:
Suprapubic catheter was also placed in the ED prior to the pt going to the OR. Another rare procedure, not required, but useful to know.
One our own Ophtho residents, Dr. Mark Mugavin (PGY-3), has started a YouTube channel where he is posting a series of Ophtho lectures as part of an education project. These lectures are designed for non-Ophtho residents who may run into eye complaints in their practice – AKA us.
So far he has 3 lectures posted, Ophthalmology ER, Pupils, and Practical Ophthalmology Trauma. I’ve watched them and found them helpful, would especially recommend them to the interns. Here’s the link to his channel:
Recently I had an interesting case at Kosair of a 5 day old male who presented with jerking movements of his arms and legs. He always had “twitches,” which the parents had been assured were normal for a newborn, but the episodes were getting worse. Since the day before, he had had several episodes where both arms would shake and seize up and his legs would curl up under him, lasting about a minute. He is sleepy afterwards, but mom thinks he’s always pretty drowsy. Overall it was unclear if what mom was describing was a seizure. Even her helpful phone videos were not 100% clear, but we proceeded as though they were real seizures. In a 5 day old.
Mom had 3 UTIs during pregnancy, and her labor was likely precipitated by an episode of pyelo. She and baby were briefly tachy during labor but pain meds helped, and the SVD was otherwise uneventful. No STIs, GBS negative.
Baby was afebrile, normal VS. Appeared drowsy until the usual screeching during the cath urine, so overall, well-appearing baby. He did twitch sometimes, but he never had one of the spells while he was in the ER.
Differential diagnosis for neonatal seizures? Bacterial meningitis, viral encephalitis, intraventricular hemorrhage, SAH, SDH, hypoxia, hypoglycemia, hyponatremia, inborn errors of metabolism, etc.
Our patient wasn’t actively seizing and labs were WNL.
Subdural hematoma (from birth) and meningitis were high on our differential. We went ahead and gave antibiotics but got a CT head before proceeding with the LP, and I’m glad we did. It turned out that he did have a subdural hematoma, likely parturitional. We elected to forego the LP, since he was afebrile and we already had a reasonable explanation for his symptoms. Neurosurgery wanted a repeat CT in 6 hours (surprise!), and neuro wanted an EEG (surprise!). He never had any of the episodes in the ER, so neuro didn’t start any antiepileptic medications. He was admitted to the PICU.
He never had any seizure activity on EEG, so neuro diagnosed him with neonatal myoclonus. Hypocoagulability workup by hematology was negative. Neurosurgery will follow up in 3 weeks as an outpatient. He was discharged after 4 days.
The other interesting discussion on this patient involved whether or not to involve CPS, since this type of injury could be seen with a shaken baby syndrome. The parents were very appropriate and there was no sign of any other trauma and negative skeletal survey, so CPS was not contacted. The overall assumption was that the SDH was secondary to birth trauma rather than any non-accidental trauma.
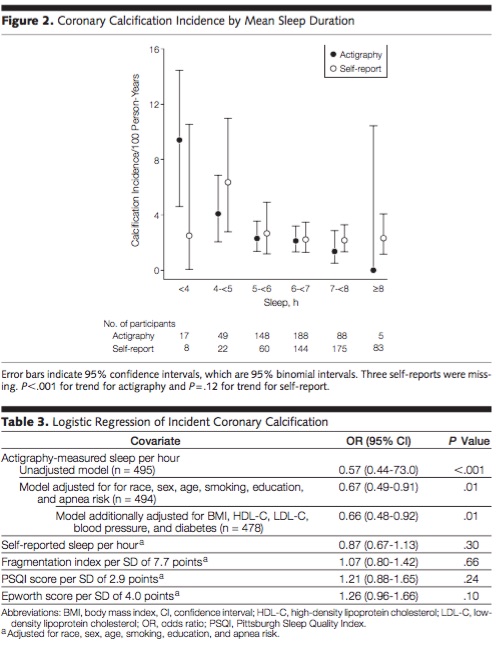
Interesting article looking at nightly sleep and coronary calcification. Pretty scary. Here is the abstract and a notable chart. They used actigraphy (wrist devices) to measure sleep and found a big difference, as many trials have, between self reported sleep and measured sleep. Sleep one extra hour a night and drop your coronary calcium by 33% (obviously this is a statistical finding and not an intervention study, still striking).
Research and Reviews in the Fast Lane (which is a must for anyone consuming FOAM) just covered a SR and meta-analysis on hypertonic saline. Relevant after our discussion in conference this morning.
Berger-Pelleiter E, et al. Hypertonic saline in severe traumatic brain injury: a systematic review and meta-analysis of randomized controlled trials. CJEM 2016. PMID: 26988719
Meet little Jimmy. No, this isn’t his real name. Jimmy has been relatively healthy for his 17 months of life. Eating and drinking has been great. No recent diarrhea or vomiting; however, Mom became worried when she noticed a rash. Yes, I said it….a rash. Initially it began as a few bumps that started to spread along his arms and legs. Sounds a little strange, eh? Here’s more background…
Let’s go back about 6 weeks prior to me seeing little Jimmy in the pediatric ED. He was prescribed Amoxicillin for otitis media. It’s a standard medication that’s given; however, he began to develop this rash around that time. No other associated symptoms though. Not pruritic and did not seem to bother him. Intermittent tactile fevers, but Mom did not associate the rash and fever. Thinking the antibiotic was the culprit, she saw the Pediatrician who said to stop taking the medication [Amoxicillin]. Pediatrician thought this could be a drug reaction.. Little Jimmy was given some OraPred and Benadryl. Told to follow up in the next several days…
Rash begins to improve over the next week or so; however, a week prior to coming to the ED, the rash returns. This time, the rash is all over the body: face, arms, legs, torso, diaper area. Continues to have the intermittent tactile fevers but the child overall seems relatively well. By this time, Mom is fed up. She’s seen the Pediatrician multiple times and has not gotten a definite answer about the rash’s etiology.
Oh yea… Mom is on a deadline too. She’s moving across the country in 1 week and NEEDS an answer.
What’s that? Describe the rash.. oh yea!
Vitals: Stable, Afebrile
General: Child is mildly fussy but consolable on examination.
Skin: Diffuse, erythematous rash along bilateral upper and lower extremities.
Scattered vesicles with occasional patches throughout extremities, most noted to the legs.
Diaper area appears erythematous, however no vesicles.
When looking at the face, a peri-oral rash is present consisting of crusted, opened vesicles. Crusting is a yellowish-golden color.
Yellowish-golden crust ….. Impetigo?
Vesicular rash along extremties with patches ….. Eczema herpeticum?
Periorificial rash affecting both mouth and diaper areae ….. Acrodermatitis enterohepathica?
Impetigo:
Causative agent(s): Staphylococci and Streptococci
Appearance: Erythematous sores that can rupture, releasing fluid or pus, and covered by a yellowish-golden crust
Treatment: Topical cream vs Systemic antibiotic treatment [Penicillins, 1st gen Cephalosporins, Doxycycline, Clindamycine]
Eczema herpeticum:
Causative agent (s): Herpes Simplex Virus, both 1 and 2, Coxsackievirus.
Appearance: Vesicles superimposed on healing atopic dermatitis
Commonly associated s/s: Fever, Lymphadenopathy
Treatment: Supportive Care, Antiviral therapy [Acyclovir]
Acrodermatitis enterohepathica
Appearance: Erythematous plaques that can evolve into vesicles and bullae
Pathophysiology: Autosomal recessive; Zinc deficiency
Treatment: Supportive care, Zinc supplementation
——
We see many rashes in the ED. Not all of them are “Viral Exanthems.” All of the mentioned “rashes” can be treated. It’s helpful to get exposure to these dermatological presentations, and it’s even more helpful to know that you can’t apply steroid cream to everything hoping that it solves the problem.
So what happened to little Jimmy?
He received IV fluids and a dose of Acyclovir. Leading diagnosis: Eczema herpeticum
What about his Zinc level? What about the wound culture?
…..Stay tuned!
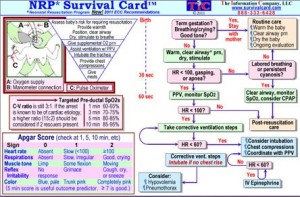
This is just a little reference card that goes along with what we learned on our last Peds Sim. I found that the Neonatal Resuscitation Program obviously has a different algorithm than with most of our resuscitation algorithms. Take a look at it, memorize it or just forget about it. Ether way here is a quick reference for everyone.