![Room9er ["Room Niner"]:](https://room9er.com/wp-content/uploads/2020/03/cropped-Screen-Shot-2020-03-08-at-3.16.16-PM.png)
Hey guys some of you were lucky enough to hear my friend Olivia Mittel and her guests educate our group in didactics. She presented information on human trafficking. This is a real issue and many of us have likely discharged a trafficking victim back into a terrible situation. Please read this Annals of EM article for more information very relevant to EM doctors.
Category Archives: Literature Reviews
Hydration
The how to stay healthy in EM posts on Aliem are definitely worth checking out. One common piece of advice given on tolerating the night shift is hydration. Here is a cool study proving this, many studies like this in the literature.
Lactate
Bosse’s favorite molecule (and lab test), lactate has a sordid and confusing history. This article in Emergency Medicine News sheds some light on lactate and its role in disease (or health). The author (Dr Paul Marik) is board certified in internal medicine, critical care, neuro-critical care and nutrition.
It may take a couple reads but this article has a succinct, common sense approach to understanding lactate production and use by the body. You may not be able to apply this knowledge on your next patient encounter, but physiology is fun right?
1.4% Observed Adverse Reaction Treated With Flumazenil
Flumazenil (Rx: Romazicon) has recently been described as coming into favor for two unique purposes: (1) hepatic encephalopathy and (2) paradoxical reactions to benzodiazepines.
Regarding the first, flumazenil’s use in hepatic encephalopathy has been well described recently in a Cochrane review of 113 RCTs with a total n = 805, wherein flumazenil had a significant beneficial effect on short term improvement of hepatic encephalopathy.1 This is thought to occur physiologically secondary to reversal of the origin of hepatic encephalopathy—i.e., an accumulation of substances that bind to a receptor-complex in the brain resulting in neural inhibition1 (principally GABA receptors which are forefront in the stimulation of sedation). Therefore GABA receptor antagonists (such as flumazenil) can be used to directly oppose this mechanism. Effect on full recovery and survival has still not been proven with flumazenil administration.1
Secondly, flumazenil can be used for paradoxical reactions to benzodiazepines2,4 and in a 10 year review of its use, published in the Journal of Emergency Medicine,3 the real safety of this drug has once again come into question, as there were relatively few adverse outcomes even in the highest of seizure provocation risk—which occurred with co administration of pro-convulsant (e.g., TCAs) at a 2.7 % incidence (8/293)—the total incidence including all subjects bore a rate of 1.4% of seizure activity (n = 904).3
I present an example of administration in the second of indications above. I took care of a 26 yo WF with PMH of asthma, a prior severe dental cavity pending root canal and an IV heroin addiction, currently sober and progressing through the the 12 Steps program at the Healing Place. She presented in sepsis, afebrile with qSOFA of 0/3 (Labs: WBC 21.2 with left shift, procal 1.33, ESR 83, CRP 201, lactic acid 0.8 s/p 2 L NS IVFs), and AKI (Cr. 1.6) with dental as well as urinary possible sources. She was eventually discharged on day 3 with Dx of urosepsis, creatinine returned to normal, and had a negative echo for routine endocarditis rule out in the setting of PMH of IVDA.
During her ER stay she was uncomfortable, diaphoretic, pale, GCS of 15, but anxious and in pain, professing severe insomnia for 3 days, stating, “I just want to sleep”. A trial of oral Ativan 2 mg was given, as she did not want any pain medication due to her prior addiction. She noted a small temporary improvement; however 2 hours later this beneficial effect was absent. By now she had received cefepime 2g and vancomycin 25 mg/kg (for potential osteomyelitis coverage), and was requesting more anxiety medications, having already received 50 mg IV Benadryl 30 minutes prior with no improvement noted. Clinically she was GCS 15, pleasant in interaction, increasingly pale, uncomfortable, wide awake at 0445, and subjectively in pain. She was then given 2 mg IV Versed.
Immediately following the administration of midazolam she became altered to GCS 12 (E4, V3, M5), eyes wide, extremities tremulous, pulled out all of her IVs, and was trying to jump off the bed. It was clear she was paradoxically agitated and hyper-aroused. Rather than reversing her (though we doubted history of benzodiazepine use), we opted to watch and see if this reaction would subside without intervention since she responded favorably to the oral Ativan; however the rarely seen but well known paradoxical reaction to Versed was suspected. She was observed 1:1 and thereafter 3:1 for 40 minutes, at which time she appeared to be steadily worsening rather than improving. The decision was made to give an IV push of 0.2 mg of flumazenil (Rx: Romazicon). Within 30 seconds after administration she once again returned to her pleasant self, she was GCS 15, appropriate, and had no recollection of the previous hour, and had no seizure activity noted throughout her stay. She maintained a healthy mental status of GCS 15 and was AAOx4 for the rest of her evaluation and admission.
In 2010, Kreshak et al. reported a similar case and treatment. This paradoxical reaction to Versed in their report is thought to occur at less than 1% incidence, however it is described as commonly as 1.4 %.4 In the reported literature this reaction is described as a patient becoming acutely agitated, restless and aggressive2. Stiffening and jerking of the extremities, and shaking of a part of the body are also noted. When observing a patient with this reaction, after ruling out other etiologies of agitated AMS, Kreshak et al. (2010) opted to administer flumazenil 0.5mg IV, and “…immediately after which the patient became conscious, oriented and calm, the paradoxical reaction was terminated”. The patient had no recollection of the events,2 similar to the patient observed in the ULED.
Per Kreshak et al. (2010), there exist “…different theories concerning the mechanism of paradoxical reactions, involving a central cholinergic effect or the serotonin imbalance”.2 Unfortunately the exact mechanism of paradoxical reactions remains unclear.
Although difficult to locate literature, if seizures develop following flumazenil administration, pharmacology guidelines recommend Valium 20-30 mg IV then immediately switching to barbiturates; some soft EM sources also suggest going straight to propofol.5
Thank you for reading my post.
References
- Als-Nielsen, B., Kjaergard, L., & Gluud, C. (2001). Benzodiazepine receptor antagonists for acute and chronic hepatic encephalopathy. The Cochrane Database of Systematic Reviews (Complete Reviews). doi:10.1002/14651858.cd002798
- Cabrera, L., Santana, A., Robaina, P., & Palacios, M. (2010). Paradoxical reaction to midazolam reversed with flumazenil. Journal of Emergencies, Trauma, and Shock J Emerg Trauma Shock, 3(3), 307. doi:10.4103/0974-2700.66551
- Kreshak, A. A., Cantrell, F. L., Clark, R. F., & Tomaszewski, C. A. (2012). A Poison Center’s Ten-year Experience with Flumazenil Administration to Acutely Poisoned Adults. The Journal of Emergency Medicine, 43(4), 677-682. doi:10.1016/j.jemermed.2012.01.059
- Tae, C. H., Kang, K. J., Min, B., Ahn, J. H., Kim, S., Lee, J. H., . . . Kim, J. J. (2014). Paradoxical reaction to midazolam in patients undergoing endoscopy under sedation: Incidence, risk factors and the effect of flumazenil. Digestive and Liver Disease, 46(8), 710-715. doi:10.1016/j.dld.2014.04.007
- (n.d.). Retrieved August 23, 2016, from http://www.goodfriendem.com/2013/05/flumazenil-romazicon-is-probably-safer.html
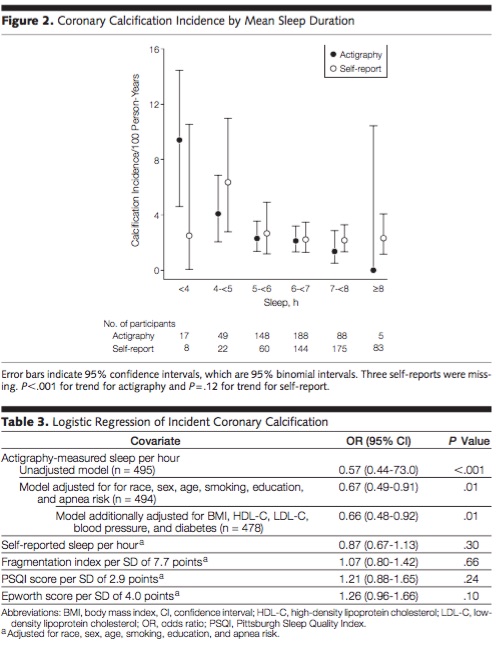
Sleep saves lives
Interesting article looking at nightly sleep and coronary calcification. Pretty scary. Here is the abstract and a notable chart. They used actigraphy (wrist devices) to measure sleep and found a big difference, as many trials have, between self reported sleep and measured sleep. Sleep one extra hour a night and drop your coronary calcium by 33% (obviously this is a statistical finding and not an intervention study, still striking).
Hypertonic Saline vs Mannitol
Research and Reviews in the Fast Lane (which is a must for anyone consuming FOAM) just covered a SR and meta-analysis on hypertonic saline. Relevant after our discussion in conference this morning.
Berger-Pelleiter E, et al. Hypertonic saline in severe traumatic brain injury: a systematic review and meta-analysis of randomized controlled trials. CJEM 2016. PMID: 26988719
- Hypertonic saline seems to be recommended more and more often for intracranial hypertension. What is the evidence in traumatic brain injury?
This is a systematic review and meta-analysis that identified 11 RCTs covering 1820 adult patients with traumatic brain injury comparing hypertonic saline to either mannitol (½ the studies) or another solution (often normal saline, or even hypotonic saline.) Hypertonic saline did not decrease mortality (RR 0.96, 95%CI 0.83-1.11). It didn’t lower intracranial pressure (weighted mean difference -0.39, 95%CI -3.78 – 2.99). And it didn’t improve functional outcomes (RR 1.12, 95% CI 0.92-1.36). Maybe we shouldn’t be rushing to adopt hypertonic saline in the management of traumatic brain injury.
- Recommended by Justin Morgenstern
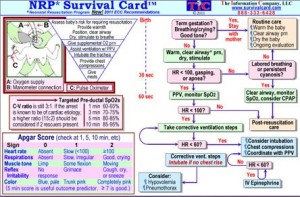
NRP
This is just a little reference card that goes along with what we learned on our last Peds Sim. I found that the Neonatal Resuscitation Program obviously has a different algorithm than with most of our resuscitation algorithms. Take a look at it, memorize it or just forget about it. Ether way here is a quick reference for everyone.
Just say NO to DESAT
I was about to spend a lot of time on a post here about pre oxygenation, specifically re: apnea oxygenation with nasal cannula. I was inspired be yet another favorable article in this month’s Academic EM (which by the way is going to be online ONLY as of Jan 2017).
Then realized Weingart had of course already posted a ridiculously good synopsis of what was out at the time.
If you plan at anytime in the future to intubate a human patient, STOP what you are doing and read the Emcrit post before your next intubation.
Add to his post the new article. And the common sense that a nasal cannula has no risk to the patient. There is just no reason not to place a 10L or greater nasal cannula on all patients during intubation.
Just finished writing the post and noticed EMLitofNote just reviewed this article, also linked to a LITFL post and a Rebel EM post. Their conclusions are similar, though they call for an RCT. Not sure we need to spend a bunch of money on an RCT. I say just use the cannula for 5 minutes while you intubate.
A Mysterious Death in a 21 yo Healthy White Female, and the Larson Maneuver
My wife is at work at a hand surgery pre-op care clinic. It is her birthday. In walks a middle-aged male who is about to have tendon reconstruction after he sustained a crush trauma, and is excited about the possibility of returning to work. He is slightly abrasive and somber, despite the prospect of receiving the surgery.
My wife asks him if he is concerned about the procedure, asks if he is feeling well, asks if there is anything she can do to help. With a quiet manner he states all is well. To make discussion my wife states today is her birthday and she is excited to celebrate when she gets home. He smiles and states today is also his daughter’s birthday. She was born the same year as my wife. He states today is always a rough day for him because she passed away in an emergency room 7 years ago at 21 years of age.
We can never fully understand where those we treat are coming from, their life experiences, or what their home situations, thoughts, fears, dreams, and worries entail; and this was a reminder for me. He stated that his daughter was healthy,woke up without issue on that day, but later developed difficulty breathing and wheezing. She was diagnosed with an acute asthma attack. She had one episode in the distant past but was not on any routine medications. She was given albuterol and experienced a negative reaction to the albuterol and completely stopped breathing. She was brain dead by the time she was intubated. They withdrew care in the emergency department.
After my wife shared this with me, I searched to find any case reports of paradoxical reactions to albuterol. Below are three related cases, however bronchospasm becoming worse with beta-blockers is exceptionally rare.
Case reports of paradoxical bronchospasm to inhaled beta agonists:
- http://www.ncbi.nlm.nih.gov/pubmed/16553105 – Paradoxical bronchospasm: a potentially life threatening adverse effect of albuterol (2006).
- http://www.ncbi.nlm.nih.gov/pubmed/18443029 – Paradoxical response to levalbuterol (2008).
- http://www.ncbi.nlm.nih.gov/pubmed/23173379 – Paradoxical reaction to salbutamol in an asthma patient (2012).
What I think more probable, and possibly related to the above case reports, is acute laryngospasm. The albuterol she received may have further irritated her vocal cords potentially worsening, rather than relieving her vocal cord dysfunction. Both Resus.me and LITFL (Life In The Fast Lane) have very useful articles describing management (see below for links). Here is a brief synopsis:
Laryngospasm
What is it?: a potentially life-threatening closure of the vocal chords (can occur spontaneously). Often misdiagnosed as asthma—especially exercise-induced asthma (more common in white females).
How to diagnose (and differentiate from asthma):
- Stridorous sounds are usually loudest over the anterior neck, beware wheezing sounds transmit throughout the lungs
- Typically, albuterol has minimal to no beneficial effect.
- Subjectively more difficulty on inspiration than expiration
Clues in history: recent exercise, GERD, ENT procedures, or extubation
Common causes & some that are not-so common:
- Post extubation
- Exercise
- GERD
- Medications (e.g., (1) ketamine sedation, incidence 1-2 %; (2) versed (very rarely), which can be reversed with flumazenil)
- Near drowning/ aspiration
- Inhalants (smoke, ammonia, dust, cleaning chemicals)
- Related to anxiety
- Strychnine (plant based poison, sometimes used as a pesticide for birds and rodents, also the poison reportedly used to kill Alexander the Great in 323 BC)
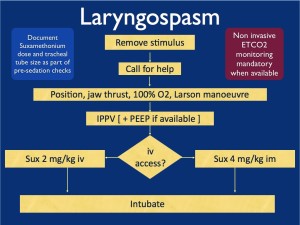
Treatment of laryngospasm:
Initially:
- Jaw thrust with Larson Maneuver
- CPAP/ NIPPV
- Heliox might be helpful if available, (also topical lidocaine can be applied to larynx if available)
If conservative measures fail:
- Low dose propofol (0.1 mg/kg) ~ give 10 mg
- Low dose succinylcholine (AKA: suxamethonium) 0.1-0.5 mg/kg IV
- All else fails: intubation with succinylcholine 1.5 mg/kg IV
- If no IV access, then succinylcholine IM (3-4 mg/kg). Experts advocate IM injection into the tongue.
- Perform chest thrust maneuver immediately preceding intubation to open the vocal cords and allow passage of the ET tube.
- Monitor for negative pressure pulmonary edema—(from patient pulling hard against closed glottis in the setting of acute asphyxia).
Flow chart from Resus.me
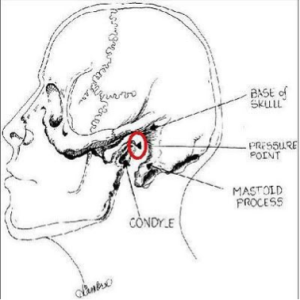
What is the Larson Maneuver? (Published 1998 in Anesthesiology)
It is a manipulation jaw thrust technique targeted at the ‘Larson’s point‘, AKA: laryngospasm notch.
- Place middle finger of each hand in the laryngospasm notch, located behind the lobule of each ear, between ascending ramus of the mandible and the mastoid process.
- Press very firmly inward toward the base of the skull with both fingers
- At the same time lift the mandible at a right angle to the plane of the body (perform jaw thrust).
Reportedly will convert laryngospasm within one or two breath cycles to laryngeal stridor, and in after a couple more breath cycles, to unobstructed respirations. As proposed by Larson, it is likely that the painful stimulus relaxes the vocal cords by way of either the parasympathetic or sympathetic nervous systems through the glossopharyngeal nerve.
Diagram from LITFL
References:
- Resus.Me: http://resus.me/laryngospasm-after-ketamine/
- LITFL (Life In The Fast Lane): http://lifeinthefastlane.com/ccc/laryngospasm/
- UpToDate: https://www.uptodate.com/contents/paradoxical-vocal-fold-motion?source=machineLearning&search=Laryngospasm&selectedTitle=1~150§ionRank=1&anchor=H3#H3
- Larson, Philip, MD. Laryngospasm-The Best Treatment. Anesthesiology. 1998. http://anesthesiology.pubs.asahq.org/article.aspx?articleid=1947036
- Paradoxical bronchospasm: a potentially life threatening adverse effect of albuterol. South Med J. 2006 Mar;99(3):288-9. http://www.ncbi.nlm.nih.gov/pubmed/16553105
- Paradoxical response to levalbuterol. J Am Osteopath Assoc. 2008 Apr;108(4):211-3. http://www.ncbi.nlm.nih.gov/pubmed/18443029
- Paradoxical reaction to salbutamol in an asthma patient. Pneumologia. 2012. Jul-Sep;61(3):171-4. http://www.ncbi.nlm.nih.gov/pubmed/23173379
Treating BB/CCB overdose
Systemic review article on treating BB/CCB overdose
CCB poisoning A systematic review
Key points:
1) High dose insulin 1u/kg bolus and then 0.2-0.3u/kg/h in conjunction w a vasopressor improves survival.
2) No mortality benefits with glucagon or atropine
3) In animal studies , lipids, levophed and dopamine improves survival
4)Consider ECMO for pts in cardiac arrest or refractory shock.
Sick PEs
We had a very ill patient recently. She was found down upstairs visiting her family member. She was calmly altered, not agitated but was in mild distress. Consciousness fluctuated. Tachycardic and hypertensive initially, then had more labile BP and some hypotension.
We had to intubate her due to poor MS and clinical condition. She coded in CT, we placed a central line on the CT table between her noncontrast head CT and her CT chest. We pushed an amp of Epi and ran out of the room for the CT chest. We were worried about dissection and PE in equal amounts. We could not get good cardiac windows on bedside Echo in room 9 prior to the CT.
She continued to intermittently lose her pulse and drop her BP. We confirmed bilat PEs on the CT when we saw NO contrast left her right ventricle. The CT tech noticed first and became worried the patient had no cardiac output (ie pulseless).
We rushed the patient back to room 9 and gave a tPA bolus (50mg) followed by infusion of 40mg. She was on pressors and heparin and improving. Dr Smith accepted her to Jewish for possible EKOS or even ECMO if needed. On arrival to Jewish a few hours later she coded and died.
I was surprised when I found out she had died. Her O2 sat was improving, HR was decreasing, blood pressure was stable (though dependent on pressors). She received a large amount of crystalloid IV which according to some data might not have been optimal management. She also had the following ECG:
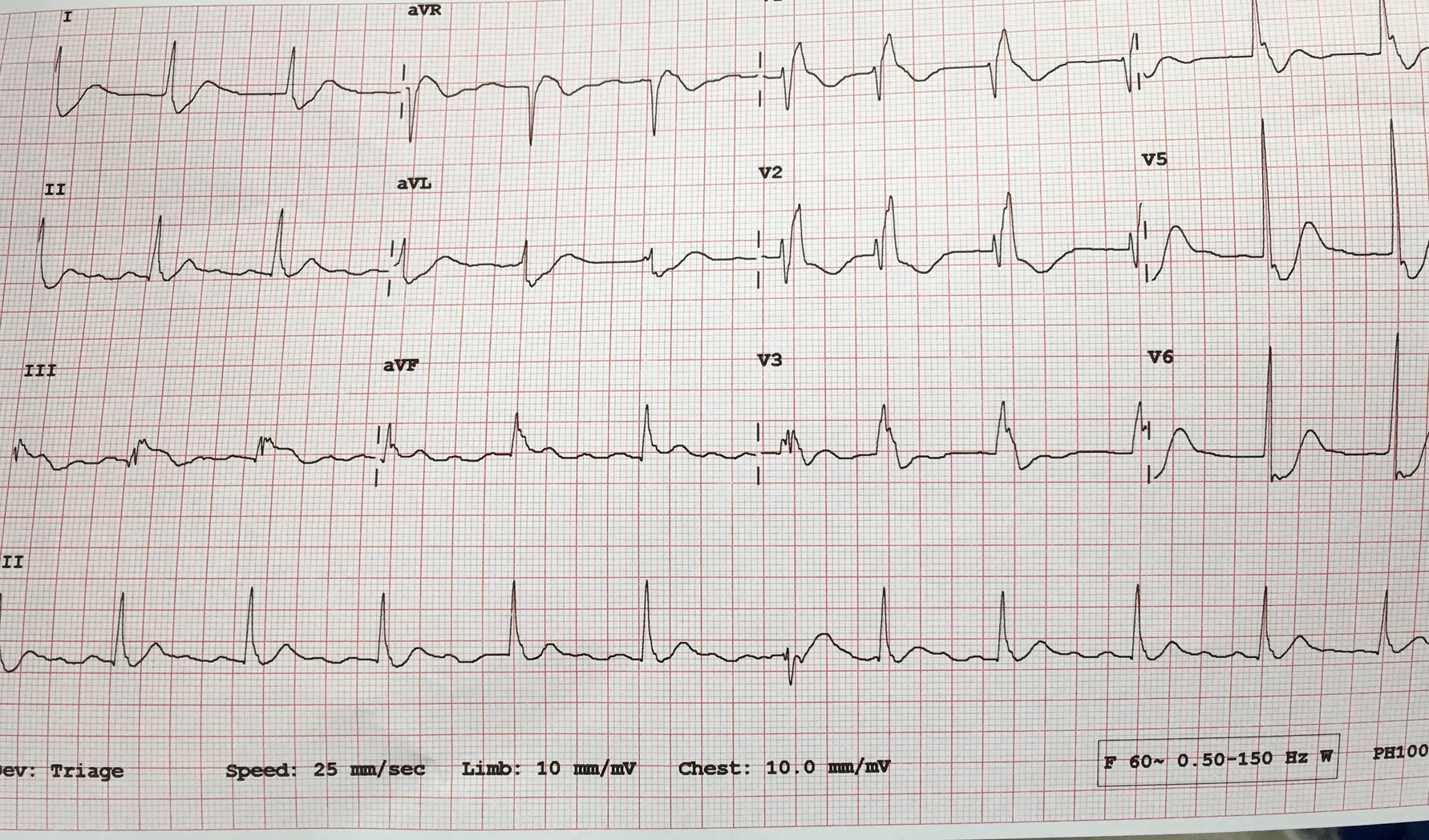
I think she was infarcting her myocardium. She likely had pulmonary infarction considering her poor oxygenation. She had coded a few times. She had a lot of strikes against her. Her BEST SHOT was going to a place with catheter assisted treatment for PE and ECMO if needed.
I am posting the case to let everyone know:
- How to manage sick PE patients (see post below)
- To use tPA in massive and in many cases of submassive PE
- TRANSFER sick PE patients to Jewish for EKOS/ECMO
- The decision to diagnose PE with RV strain on BEDSIDE Echo with no formal Radiologic testing will depend on your attending
This post from EmCrit / PulmCrit is a beautiful summary with potential dogmalysis related to PE management (see take home points below but do read the post).
In addition, here is a nice review article on catheter-based reperfusion treatment for PE with nice references for further reading.
Take home points from the Emcrit post:
- The only evidence-based intervention that seems to improve mortality in massive PE is thrombolysis. The primary goal of therapy should be administration of thrombolysis as soon as possible to patients without contraindication.
- Consider early stabilization of blood pressure using a norepinephrine infusion, administered peripherally if necessary.
- Volume administration may facilitate dilation of the right ventricle and hemodynamic deterioration.
- Intubation is very hazardous and should be avoided if possible. Patients die from cardiovascular collapse, and intubation may worsen this.
- For a coding PE patient consider 50mg alteplase bolus as well as an infusion of epinephrine. Patients can do well despite requiring CPR and high dose vasopressor infusions.
Phrenic Nerve Paralysis after intrascalene nerve block
This was covered in the opening of the February EMRAP however not something that I was at all familiar with. Here are the basics and something that is probably rare but worth knowing about:
In the episode they presented a case of 70 year old female that was brought in with a complaint of shortness of breath. RR = 28 and SA02 – 88%. The patient presented three hours after a right shoulder arthroscopy.
ECG : normal
CXR: elevation of the right hemidiaphragm
Dx: paralysis of right hemidiaphram after intrascalene nerve block
There are two major complications associated with intrascalene nerve blocks: 1. pneumothorax
2. unilateral phrenic nerve paralysis.
The patient likely had a transient phrenic nerve dysfunction causing unilateral diaphragmatic paralysis. Younger patients can compensate, older patients with co-morbid conditions may not be able to tolerate this as only one lung is effectively ventilating.
The patient in this case was managed with supplemental 02 until the buvipicane wore off. Some patients with underlying lung disease and this complication may require BiPAP/CPAP or intubation.
Things that I took away:
- be aware of this procedure and this complication
- this may be done for patients with same days surgeries to the upper extremity and this is important history to have from Pt or family.
- It may be missed prior to d/c. This was an example of one that was missed by Anesthesia prior to d/c of the patient.
- May look clinically like PE (tachypnea, tachycardia, post-op patient), however, history will help make the dx as well as CXR.
A little more about the block:
Interscalene nerve block is typically performed to provide analgesia for upper extremity surgeries and may or may not be combined with mild general anesthesia.
Example of Surgeries this may be used for:
-Shoulder surgery, such as rotator cuff repair, acromioplasty, hemiarthroplasty, and total shoulder replacement
– Humerus fracture
Drug Interactions
Not sure if anyone follows David Juurlink on Twitter. He posts a lot on the opioid epidemic amongst other pharm and to topics. Here is a lecture on dangerous drug interactions. You can watch the video or skim the slides.
Valsartan/sacubitril use likely to increase significantly
So I just came across that the Valsartan/sacubitril (Entresto) was given a strong class 1 recommendation by the American College of Cardiology for heart failure. I haven’t seen much of it in med-recs yet, so I just wanted to post a couple of high points that I think we need to know from the ER side. From what I’m reading this drug will start to replace ACE-Inhibitors in the treatment of Class II-IV heart failure. It’s also prescribed in slightly odd dosing in the combination (51 mg/49 mg or 26 mg/24 mg).
Sacubitril is a prodrug that converts to sacubitrilat. Sacubitrilat is responsible for the benefits of this drug as it inhibits the enzyme neprilysin and stops it from degrading atrial/brain natriuretic peptide.
Ultimately the main thing you need to know are the contraindications with other drugs. Basically there are 3: Lithium, ACE-Is, and Aliskiren. Lithium levels have the potential to increase with this drug, while the other 2 can lead to significant hypotension in combination with Valsartan/sacubitril.
Here’s the ACC release: http://www.acc.org/latest-in-cardiology/articles/2016/05/20/11/30/societies-release-focused-update-for-hf-management?wt.mc_id=fb
Would be appreciate if someone with a stronger background in pharmacy or cardiology than I can chime in.
Urine Drug Screen
So while on my ICU months this year, I had upper levels that were very insistent that we needed to get a urine drug screen on everyone. I would try to make the point that it most likely was not going to change our management of the patient at all. My point was often ignored and after countless urine drug screens obtained during those months, most if not all proved to be of no utility.
Interestingly, Foamcast just put out a podcast about false positives and false negatives on the UDS. What I found most interesting was that ibuprofen can cause a false positive for just about anything under the sun including cocaine, PCP, THC, and barbiturates. Also, the benzos tested on this really only test for oxazepam which is a metabolite of diazepam. So Ativan, Klonopin, and Xanax won’t show up.
Here is the link if you want to read the whole thing. https://foamcast.org/2016/04/26/episode-48-urine-drug-screen-cocaine-and-pcp/