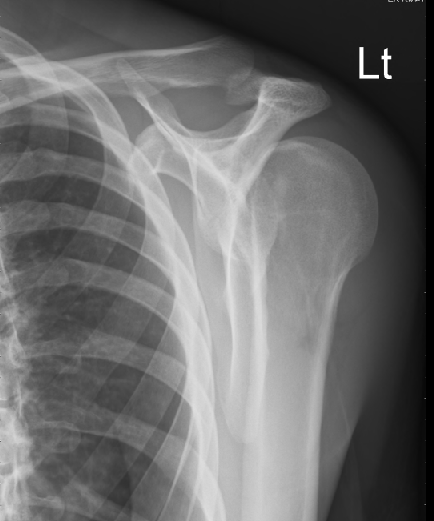
Young male with history of psychiatric illness and seizures presents with left arm pain after a fall. Patient thinks he slipped on ice, but is unsure. He reports no LOC, no head pain, no neck pain. Does not believe he had a seizure. No urinary incontinence, no tongue biting. Has severe pain in left shoulder. Physical exam shows small forehead abrasion, no c-spine tenderness, and decreased ROM to left shoulder. He holds his arm internally rotated and adducted. There is an obvious deformity to the left shoulder with a defected palpated anterior.
3 view x rays ordered in triage read as negative for fracture or dislocation, but limited by poor patient positioning.


I was pretty sure that it was dislocated, so I went ahead and ordered the definitive axillary view.
As I was charting on another patient, the x-ray tech came over, looking slightly embarrassed, and said that she was pretty sure she had just reduced my patient’s shoulder as she was trying to get him in the proper position for the axillary view. She said, “It was amazing, he couldn’t move it, then pop, and he has full ROM now.”
Nice.
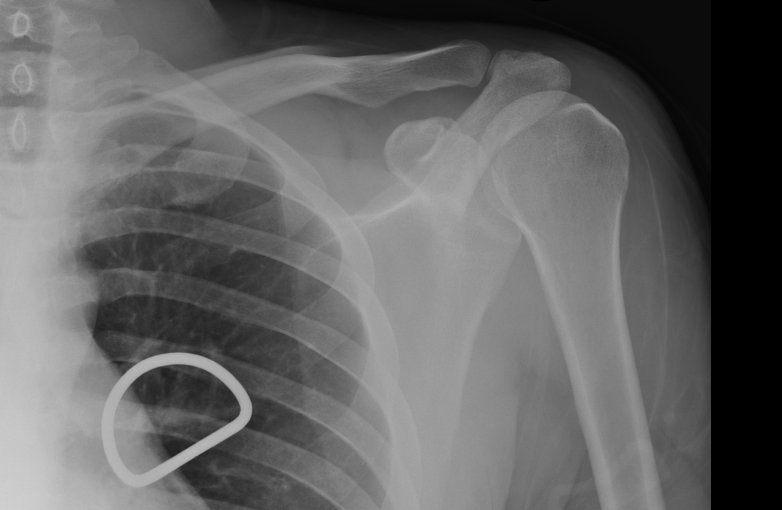
Two minutes later, got a phone call from radiology…Might have missed a posterior dislocation…Looks great in the axillary view now…Would recommend getting repeat normal films to be sure that there was no fracture missed while it was not in proper position.

Ordered the repeat 3 view x-rays and went to make sure he was still reduced. Found my patient still internally rotated, in pain, not able to move, and still with the hollow anteriorly. Gently held his hand and arm and before he realized what I had done, pulled slightly and externally rotated and put it back in place. As I called for the sling, he went to take his gown off and it slid back out as he extended his arm and moved it anteriorly. Tried again to gently externally rotate it, but he was now on to me and and was tense and pulling against me. Asked for suggestions other than sedation and got one from the one and only Dr. Martin Huecker: Try the Cunningham technique.
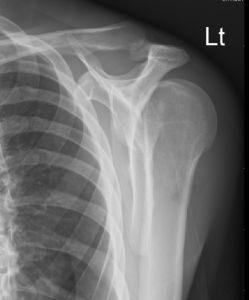
I went back in his room. He was looking a little wary. I told him it’s not going to hurt; I was just going to massage his arm a little bit to see if it will go back in. I held his left forearm in my left hand at the elbow and, using my right hand, massaged first his trapezius, then his deltoid, then his biceps, then his deltoid, then his trapezius, then his deltoid ….annnnnnnnnnnnd….. it slid back in place. Patient looked as surprised as I did. Immediately put him in a sling and swathe. Got repeat x-rays in the sling.



He was in the department for about 30 minutes after that while awaiting x-ray reads and his arm stayed reduced while in the splint. No fractures on x-ray. He was discharged with orthopedic follow up in the sling.
One can find is a formal description of The Cunningham technique from the blog “Life in the Fast Lane.” http://lifeinthefastlane.com/cunninghams-shoulder-relocation/
- Inform the patient of the procedure and the fact that it will be painless. It is important to relax the patient and confident reassurance is the first step towards this.
- Sit the patient up with the back vertical. This can be done on a bed, chair or trolley, but preferably seated on a non-wheeled chair without arm rests.
- Carefully support the arm while it is moved into the correct position, allowing the patient to help with the other arm. The correct position is with the arm adducted (next to the body) and pointing vertically down, the elbow is flexed at 90 degrees so that the forearm points horizontally and anteriorly.
- The operator then squats/kneels to the side of the patient and facing the opposite direction to the patient. The operator then slips the hand between the patients forearm and body so that the patient’s wrist/hand is resting on the operator’s upper arm. Do not make pulling movements at any time as this will elicit pain and result in spasm.
- Apply steady, very gentle traction (the weight of the operators forearm is quite enough) directly downwards once the patient is settled and pain free. Keep this gentle weight on the arm throughout, stop if any spasm or pain. Usually resting with the patients arm in this position will start to reduce the pain of spasm.
- With the other hand, the operator then massages the trapezius, deltoid and biceps muscle sequentially, repeating this process and concentrating on the biceps brachii until the muscles are fully relaxed. A strong kneading of the biceps with the thumb anterior and the four fingers of the operator posterior to the arm is recommended. At this point the humeral head will relocate usually without any clear indication that the shoulder has reduced (no sound or ‘clunk’ feeling). This means that the shoulder must be observed/checked regularly to confirm when relocation has occurred (with shoulder exposed movement can be seen as the ‘step’ disappears.)
And a link to the blog with the description. It has a nice video.
![Room9er ["Room Niner"]:](https://room9er.com/wp-content/uploads/2020/03/cropped-Screen-Shot-2020-03-08-at-3.16.16-PM.png)