PECARN = cohort of 20+ large academic institutions that combine to produce academic research studies
ciTBI = clinically important traumatic brain injury
Want to have high sensitivity = screening test = rule out ciTBI and need for CT scan
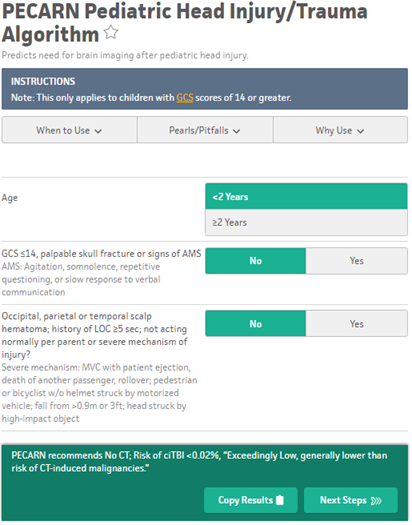
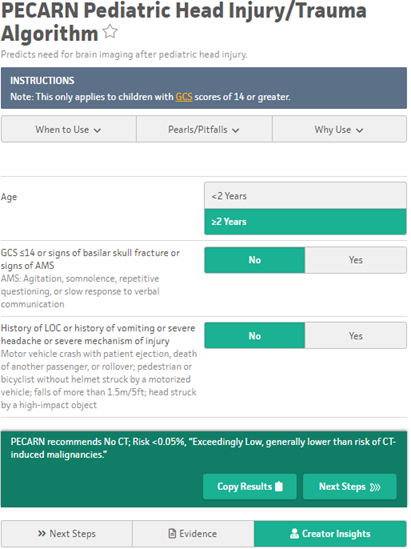
PECARN Criteria:
Age: <2 yo or >2 yo
GCS ≤14 or signs of basilar skull fracture or signs of AMS
AMS = Agitation, somnolence, repetitive questioning, or slow response to verbal communication
History of LOC or history of vomiting or severe headache or severe mechanism of injury
Small children = severe fall > 3 ft
Older children = severe fall > 5ft
Observation vs CT scan
Observation usually 4-6 hours; may take into account time from injury
Children with no PECARN criteria ciTBI predictors = lots of head CTs which could be avoided
Recommend repeat physical exam prior to discharge if observation
Conclusion:
Severe injury mechanism
Children with isolated severe injury mechanism are at low risk of ciTBI, and many do not require imaging.
Scalp hematoma
Clinicians should use patient age, scalp hematoma location and size, and injury mechanism to determine need for imaging in otherwise asymptomatic children.
VP shunt
Children with VP shunts had higher CT use but similar rates of ciTBI compared with children w/o VP shunts. (limited sample size)
Image Source: MDCalc
Peritonsillar abscess
Presenter: Dr. Brett Nelson
Most common deep space infection of head and neck
Predisposed by previous/recurrent tonsilitis or pharyngitis
Symptoms:
Odynophagia, drooling, voice change
Evaluation:
Edematous tonsil, pillars, or soft palate
Uvula deviation
Ultrasound
Intraoral US with endocavitary probe
Submandibular US with linear probe
CT head/neck w/ contrast
Treatment:
Needle aspiration – start near superior tonsillar pole, cut needle guard to protect
Incision and drainage – cut scalpel guard to protect
Antibiotics alone – Augmentin +/- Clindamycin
“Quinsy Tonsillectomy” – performed by ENT in severe cases of airway obstruction
Disposition: Usually discharge with ENT follow-up
Sialolithiasis and Suppurative Parotitis
Presenter: Dr. Kyle Stucker
Sialolithiasis:
Calcium carbonate or phosphate stones of salivary gland in stagnant duct
Here are four papers on ovarian torsion. If you suspect torsion clinically, do NOT be reassured by normal flow on USN. Only the last paper (12 years old) showed a high sensitivity of ultrasound doppler flow for torsion. The other findings matter!
20 cases, 20 controls. Pelvic US for ovarian torsion was 80.0% sensitive (95% CI, 58.4-91.9%) and 95.0% specific (95% CI, 76.4-99.1%) for reader 1, while 80.0% sensitive (95% CI, 58.4-91.9%) and 85.0% specific (95% CI, 64.0-95.0%) for reader 2.
55 cases of surgically proven torsion, 48 controls. Sixty-one percent of right ovarian torsion case and 27% of left ovarian torsion cases had normal Doppler flow. Presence of ovarian cysts was significantly associated with torsion. Sensitivity of ultrasound was 70% and specificity was 87%.
One hundred and ninety-nine patients presented with adnexal mass and intermittent lower abdominal pain. Sensitivity and specificity of tissue edema, absence of intra-ovarian vascularity, absence of arterial flow, and absence or abnormal venous flow in the diagnosis of adnexal torsion were: 21% and 100%, 52% and 91%, 76% and 99%, and 100% and 97%, respectively. All patients with adnexal torsion had absent flow or abnormal flow pattern in the ovarian vein. In 13 patients, the only abnormality was absent or abnormal ovarian venous flow with normal gray-scale US appearance and normal arterial blood flow. Of these 13 patients, 8 (62%) had adnexal torsion or subtorsion.
TL;DR
1. Ovarian Torsion is a clinical diagnosis. Ultrasound is NOT 100% sensitive.
2. Read the USN report, Just like a cardiac cath*, normal must really mean normal. If you can’t visualize one ovary, or have normal ovarian flow but a large cyst, or have edema, etc, that is NOT a normal pelvic ultrasound.
* A cath report that has 50% blockage in 2 vessels is not “normal” or “clean”! Caths with absence of a lesion that requires PCI (stent) can still have abnormalities that are very important. Remember, the 50% coronary plaques are the most likely to be unstable and rupture.
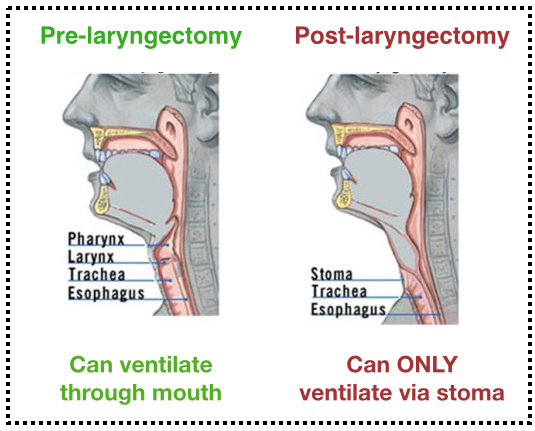
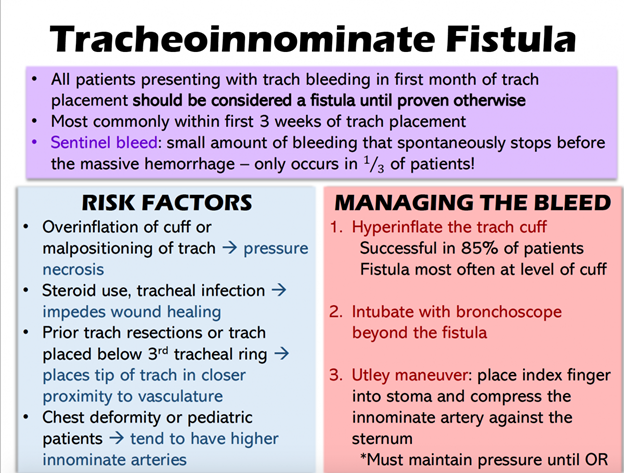
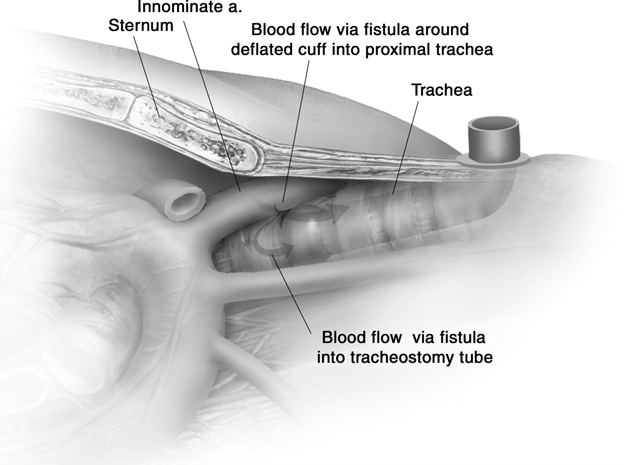
2. Consider replacing trach with standard ET tube and then hyperinflate ET tube cuff (may help if bleed is further down)
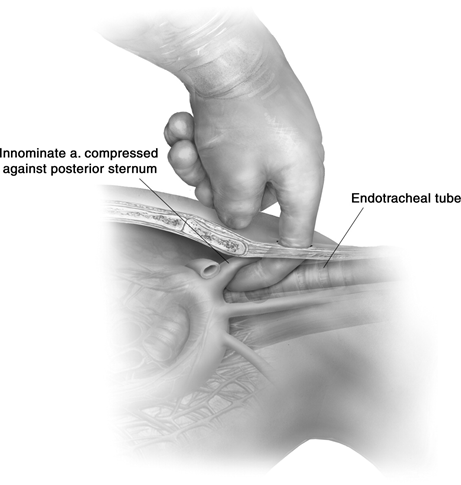
3. Insert fingers in trach site and apply pressure anteriorly against back of sternum
Image Source: Ailawadi G. Technique for managing Tracheo-innominate artery fistula. Operative Techniques in Thoracic and Cardiovascular Surgery. 2009;14(1):66-72. doi:10.1053/j.optechstcvs.2009.02.003
Image Source: Ailawadi G. Technique for managing Tracheo-innominate artery fistula. Operative Techniques in Thoracic and Cardiovascular Surgery. 2009;14(1):66-72. doi:10.1053/j.optechstcvs.2009.02.003
Lighting Lectures:
Presenter: Dr. Jordan Martinez and Dr. Adam Lehnig
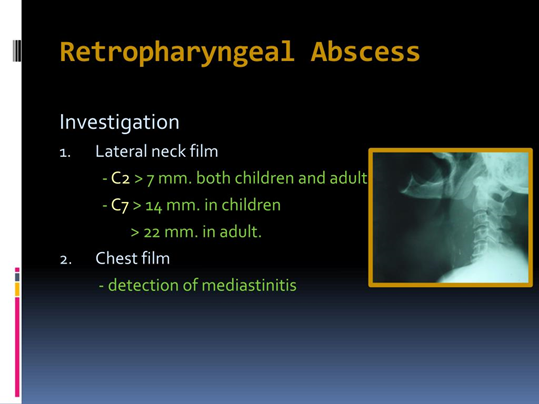
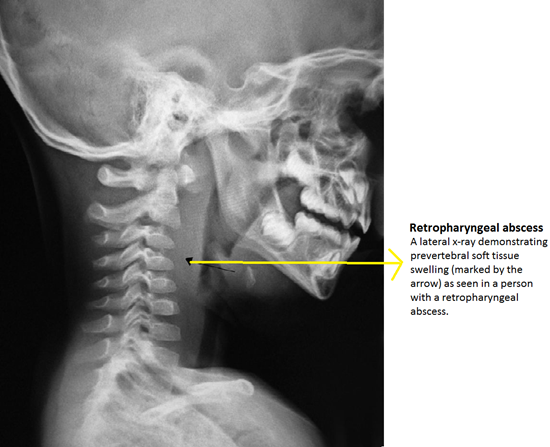
Retropharyngeal Abscess
Age: 2-4 years old most common
Often presents after an infection, usually URI
May be precipitated by trauma, dental procedure, intubation, etc
Polymicrobial infection
Management:
Evaluate for airway compromise –> ABCs
Obtain CT soft tissue neck W (historically lateral neck X-ray was used)
Evaluate for signs of respiratory distress: drooling, dyspnea, dysphonia, dysphagia
Fiberoptic nasal intubation if necessary
Consider CT imaging
Antibiotics: IV Unasyn – first line
Polymicrobial infection – consider broad spectrum if known MRSA or pseudomonal exposure
ENT consult
Room 9 Follow-Up:
Presenter: Dr. Dylan Nichols
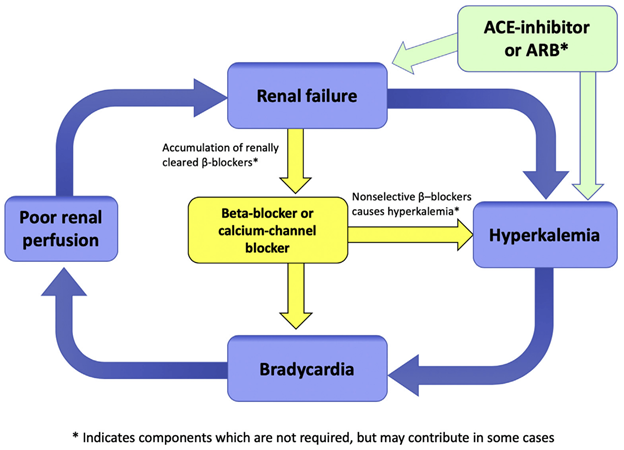
Two patient cases discussed. Both patients with bradycardia in the setting of acute renal failure and severe hyperkalemia. Both patients demonstrated transient bradycardia which eventually resolved.
BRASH Syndrome:
Bradycardia
Renal Failure
AV blockade
Shock
Hyperkalemia
Consider in: Elderly patients with cardiac disease on BB/CCB
Trigger: hypovolemia or AKI
Image Source: https://litfl.com/brash-syndrome/
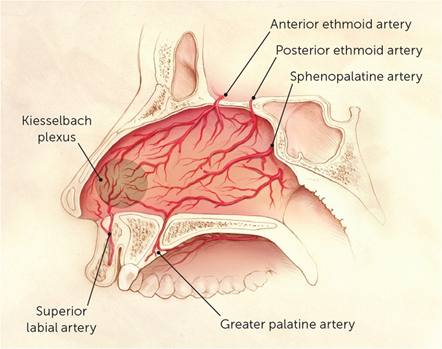
Epistaxis
Presenter: Dr. Matthew Eisenstat
Anterior Bleed (90%): comes from Kiesselbach’s plexus
Posterior Bleed: (10%): higher concern severe bleeding or arterial bleed (sphenopalentine artery)
Position the probe over posterior aspect of affected shoulder with indicator to patient’s left
Measure distance between glenoid and humeral head
Advantages: faster than XR, ~100% sensitivity
Disadvantages: less sensitive for fractures, operator dependent, not full agreement on measurements
Fascia iliaca compartment block (FICB)
This is different from the “femoral nerve block” and “3 in 1 block”
FICB anesthetizes femoral nerve and lateral femoral cutaneous nerve
Target: facial plane above the iliacus muscle. Infrainguinal.
Inject 30-40 mL medial to femoral nerve using a 21 or 20 gauge spinal needle and extension tubing
0.2% or 0.5% Ropivacaine or Bupivacaine
Analgesia onset within 30 min and lasts ~12 hrs
If using 0.5% dilute 20 mL anesthesia with 20 mL NS
ALWAYS calculate your dose
PE Clinical Pathway
Categorization
Massive: hypotension
Submassive: RV dysfunction or myocardial necrosis w/o hypotension
Non-massive or Sub-segmental: no hypotension, RV dysfunction, myocardial necrosis
Utilize PERC and Wells criteria
See full pathway posted separately
Extremity Trauma by Dr. Caleb Davis
Clavicle fx – typically manage with sling
May need OR if there is skin tenting or blanching
Beware of scapulothoracic dissociation in AC joint injury. Requires OR
Luxatio erecta (inferior dislocation) – to reduce, push the humeral head anteriorly under traction and then reduce like an anterior dislocation
Scaphoid fracture – MRI is best imaging modality in the acute setting
Pelvic ring injuries a thorough rectal and vaginal exam is indicated to rule out hollow viscus injury from the bone.
Hip dislocation – need post-reduction pelvic CT to look for fracture fragments
Femoral shaft fractures
associated injuries common
Need to make sure patient is adequately resusicated prior to operation to avoid 2nd hit injury to lungs. Get lactic and ABG to measure resus. Place on 2L NC.
Don’t miss open fractures. Can be small “poke-hole”
Knee dislocations – get ABG and CTA
Tibial plateau fractures are often too swollen to fix initially.
Fractures 2/2 GSW from 9mm rounds or lower are not considered open fractures
Compartment syndromes
pain out of proportion (first symptom)
pain with passive stretch (most sensitive finding)
Clinical diagnosis
Airway Assessment and Interventions
Sedation/RSI
Depth of sedation: mild, moderate, deep, general anesthesia
Risk assessment with ASA class and LEMON
SOAP-ME
Suction
Oxygen- preoxygenation and apneic oxygenation
Airway equipment
Positioning – put the towel roll under the occiput (NOT the shoulder) to align the tragus and sternal notch. Consider ramping the patient.
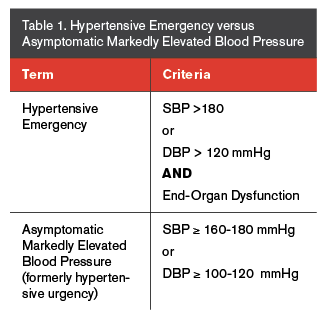
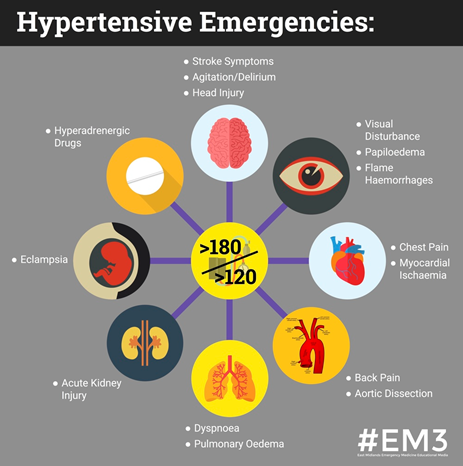
I have recently seen many patients sent to the ED from urgent care centers and PCP offices for evaluation of hypertension. While true hypertensive emergency often leads to straight forward disposition, this condition is rare and much more commonly patients present with severe asymptomatic hypertension (sometimes referred to as hypertensive urgency). I will discuss an approach to management of these conditions below.
Treatment with IV anti-hypertensives and admission to appropriate service, usually medicine or cardiology.
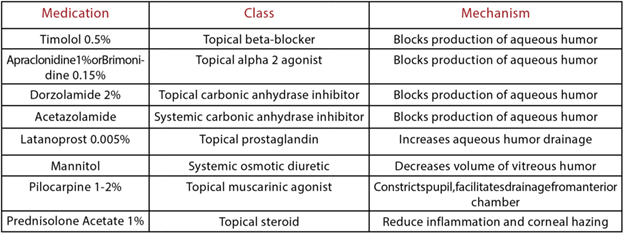
Common IV anti-hypertensives:
labetalol IV push (5-20 mg)
hydralazine IV push (10-20 mg)
nicardipine drip (start at 5 mg/hr and titrate to goal BP)
nitroglycerin drip – specifically for acute pulmonary edema (see SCAPE management for dosing)
BP Goal: reduction in MAP by 10-20% in the first hour followed by gradual reduction in MAP by ~25% over the first 24 hours. Commonly a goal BP of ~160/100 achieves goal of 10-20% reduction.
*There is increased risk of cerebral and cardiac ischemia if lowering BP too rapidly
Exceptions:
Hemorrhagic CVA and aortic dissection have specific guidelines for BP goals and rapid lowering
Ischemic CVA allow for permissive hypertension
*Beta-blocker contraindicated in amphetamine intoxication and pheochromocytoma
amphetamine intoxication – use benzodiazepine
pheochromocytoma – use alpha-blockers (phentolamine)
Severe asymptomatic hypertension (hypertensive urgency): Severe hypertension, commonly defined as BP > 180/120, with no signs of end-organ damage.
*Some physicians strongly dislike the term “hypertensive urgency” and ACEP utilizes the term “asymptomatic severely elevated blood pressure”.
This is a diagnosis of exclusion. As an ED physician it is your job to first rule out hypertensive emergency.
Management of severe asymptomatic hypertension:
* The first 3 steps below should apply to any patient presenting for hypertension.
Place patient in a quiet and relaxing environment (when possible)
Administer patient’s home PO anti-hypertensives if not taken today
Control patient’s pain and treat any underlying causes
Consider additional PO or IV anti-hypertensives
PO anti-hypertensives
Captopril (6.25-50 mg)
Enalapril (2.5-20 mg)
Clonidine (0.1-0.2 mg) *Would avoid due to variable response
IV anti-hypertensives
labetalol IV push (5-20 mg)
hydralazine IV push (10-20 mg)
BP reassessment following administration
Goal BP prior to discharge:
Ideally BP ~160/100
In a completely asymptomatic patient, BP ~180/110 or even higher may be acceptable with appropriate follow-up
No definitive recommendation exists for a blood pressure cut-off for which an asymptomatic patient must be acutely treated
Many physicians have personal practice patterns and different comfort levels with this
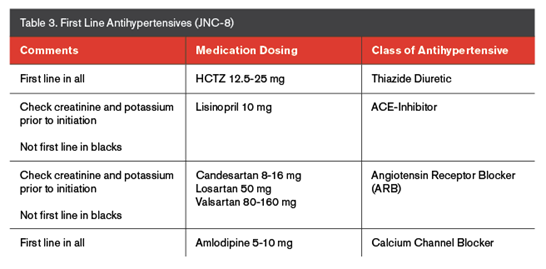
Discharge Medications:
If initiating home PO anti-hypertensives common medications include:
Amlodipine (5-10 mg)
Hydrochlorothiazide (HCTZ 12.5-25 mg)
May considering increasing current home anti-hypertensive dose but would avoid this in most circumstances
Once again, many physicians have personal practice patterns and different comfort levels with initiating or increasing doses of antihypertensives from the ED
Presence of fat pads can indicate underlying fracture
Posterior is always pathologic.
A thin anterior fat pad is normal, but a “sail sign” is pathologic
Management of common fractures
Monteggia fracture – urgent ortho consult for ORIF
Seymour fracture – physeal fracture of distal phalanx with associated nailbed injury. High risk for soft tissue entrapment. Requires Hand consult for likely ORIF
Tufts fracture w/ nailbed injury – antibiotics not required. Follow-up in 7-10 days with Hand
Common avulsion fractures (e.g. ASIS, lesser troch, iliac crest apophysis avulsion) should be NWB on affected extremity and f/u with ortho.
Torus fracture – splint with short arm cock-up splint
ABEM exists to verify the abilities of physicians and to promote quality, trust, and responsibility.
They aim to make our board certification more valuable by advocating for our value in hospitals
See ABEM website for details about board certification and the exam
Study for your exam!
Small Group: Nail bed Infections
Flexor tenosynovitis
Hand emergency. Pt will often require OR washout with Hand surgery.
Paronychia
Manage with warm compress and/or I&D
Subungual hematoma
Ensure there is no underlying fracture
Trephination is generally reserved for symptomatic treatment within the first 24hrs
HIPAA: common scenarios and what is appropriate
Family member: provider may disclose “directory info” (patient location and general health status) if caller identifies the patient by name.
The provider must first provide the patient with opportunity to agree or object
Personal physician
Disclosures of PHI from one provider to another for treatment purposes are permissible without the patient’s authorization. Disclosing provider must use professional judgement to determine whether the requested PHI relates to the patient’s treatment by the requesting physician
Press
Location and general health status can be disclosed if requestor identifies the patient by name, unless the patient has objected to such disclosures
Can’t just ask about the status of a GSW
Test results
Provider must use their judgement to infer from the situation that a patient does or does not object
Law Enforcement
Limited situations – PHI about a patient who is suspected to be a crime victim and the patient cannot agree to disclosure; the provider may disclose the PHI if (1) she/he determines that disclosures is in the patient’s best interest and the law enforcement officials represent that the PHI needed to determine whether another person violated the law. (2) The PHI is not intended to be used against the patient. (3) An immediate law enforcement activity depends on disclosure.
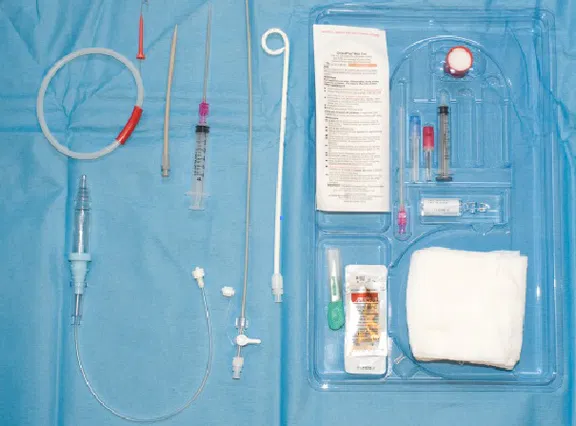
Large-bore chest tubes are still recommended for more viscous effusions such as empyema or hemothorax
Step-by-step Guide:
Prepare the chest tube atrium and ensure appropriate length tubing is available for low wall suctioning once the procedure is complete
Place the patient in either a lateral recumbent or supine body position with the head of the bed elevated to 30-45 degrees, or in a seated position with the patient leaning slightly forward for posterior tube placement (i.e. tube placement for drainage of pleural effusions, ultrasound guidance is recommended for posterior tube placement similar to with thoracentesis both to identify the location of the effusion and due to the increased presence of vascular structures between the rib spaces posteriorly)
Identify the location of insertion, usually the 4-5th intercostal space at the mid-axillary line (similar to large-bore chest tube placement) at the level of the nipple. Remember the “safety triangle” bordered by the lateral edges of the pectoralis and latissimus dorsi muscles where there is a decreased risk for damage to underlying vascular, nervous, and organ structures
Sterilize the skin surrounding the site of insertion and drape the patient accordingly using the drape provided in the kit, or by using sterile towels if preferred (remember to leave the nipple exposed to assist with identifying landmarks during catheter placement)
Measure the small-bore catheter in front of the patient’s chest to determine the appropriate depth of insertion in a manner which ensures placement towards to superior aspect of the chest with all side ports within the pleural cavity (remember, the catheter can be withdrawn but not inserted further once the procedure is complete, similar to placing a central venous catheter)
Generously anesthetize the skin at the desired site of insertion, advancing your needle deeper over the superior aspect of the rib to minimize the risk of damage to the neurovascular bundle, withdrawing prior to injecting lidocaine as the needle progresses through the soft tissue. Be sure to anesthetize the parietal pleural during this process, as it is fine for the needle tip to pass into the chest cavity
Gently advance the finder needle over the superior aspect of the rib through the intercostal musculature similarly to the previous step while steadily drawing back against the syringe plunger as the needle tip advances. The plunger pressure will give way once access into the pleural cavity is achieved. Consider loading the finder needle syringe with several mL of sterile water for visualization of air bubbles in the syringe to assist with this step
Once access to the pleural space has been achieved remove the syringe from the finder needle and insert the guide wire into the back of the finder needle passing the wire into the pleural cavity in such a manner that leaves most of the wire hanging outside of the patient
Remove the needle from the patient and make a small incision in the skin at the base of the guide wire using the provided 11-blade scalpel
Pass the dilator over the guidewire and into the pleural space feeling it give-way once it has pierced the parietal pleura and entered the thoracic cavity. Be sure to visualize the guide wire exiting the back of the dilator prior to insertion to ensure the wire is not accidentally lost within the chest. The dilator may be removed once this step is complete
Pass the small-bore catheter within its trocar over the guide wire and into the pleural space in a manner that ensures all side ports are within the space. Generally, the first black indicator line can be used for small and thin patients, the second black line for the average adult, and the third black line for large adults. Similarly to the above step, ensure the guide wire is visualized exiting the back of the trocar prior to insertion.
Dr. A. Ross, MD POC Troponin will be leaving the ED High Sensitivity Troponin (hsTnl): Less than 15ng/L in females and less than 20ng/L in males is interpreted as negative; anything above is considered positive. -Reported in whole numbers-Significant delta is an increase in 15 ng/L (over 2 hours); note a fall greater than 15 is significant too. -Must Repeat in 2 hour intervals-Will take about 30-45 min to result. T2 Bacterial PCR: rapid diagnostic ecoli, s. aureus, klebsiella, pseudo, E. faecalis-TAT 3-5 hours Who: septic patients Benefit?: Deescalation of antibiotics once resulted.
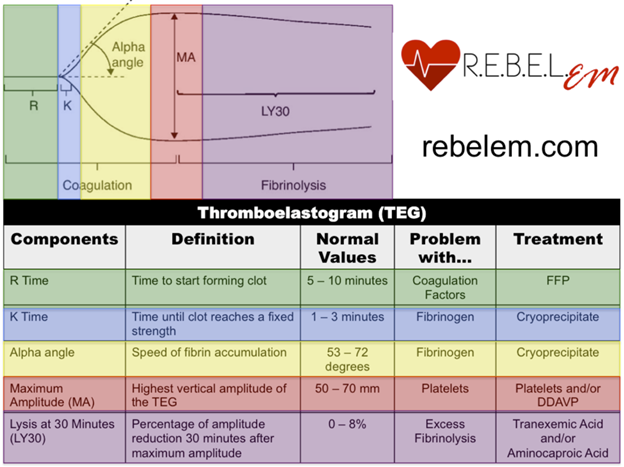
Level 1 Activation Criteria: SBP <90mmHg, Resp compromise or impending, EP Discretion, Blood resuscitations to maintain VS in transport, GSW or severe penetrating trauma to neck, chest, or abdomen, GCS <9 with mechanism attributed to trauma.NOTE: GSWs to the head and going to SICU (call trauma on these) do not need to activate Level 1 on these. Shunt Series: power plan in cerner; rad VP shunt series (orders all plain films) TEG Stay Tuned Continue to place Intend to Admit Order in Cerner on people you know will admit.
One Pill Can Kill
Dr. R. Lund, MD
CCB, TCA, Lamotil, Opiates/Opioids, Camphor, Clonidine, Antimalerials Opioids: Naloxone dosing peds: 2mg IV q3-5BB Tox: hypoglycemia and bradycardia; glucagon and or high insulin protocol (consult tox.)CCB: Dihydro and Non-Dihydro; Txt: supportive care; Poison Control ConsultationOil of Wintergreen: Salicylate Toxicity; Toxidrome: Nausea, Vomiting, Tinnitus, Txt: Urinary Alkalization Sulfonylureas: Admit for 24 hours, give either PO or IV. Txt: Octreotide infusion Clonidine/Imidazoles: A-2 agonist, high dose narcan and supportive care measures. symptoms: lethargy and or coma typically. Camphor: Txt: Benzos and Phenobarb for seizures; TCA: CNS, anticholinergic, and QRS prolongation; QRS 100ms< is pathologic; Tx: Benzos and Bicarbonate, Lamotil; loperamide +/- atropine; symptoms: anticholinergic and opiate toxidrome picture; txt: narcan Toxic Alcohols: Ethylene Glycol, Methanol, and Isopropyl Alcohol (rubbing etoh): Isopropyl: ketonuria; supportive care Methanol: de-icers, HA, Metabolic acidosis, breaks down into formic acid, give fomepizole or ETOH to compete out A. dehydrogenase Eth. glycol: txt: fomepizole, dialysis, and bicarb for acidosis.
SJS/TEN Dr. Slaven, MD
SJS <10%; TEN 30%<Hx physical exam key; Workup: CXR, CBC, CMP ESR/CRP SCORTEN Score predictor availableRemove inciting factor Pathogenesis: Sulfa drugs; typically first 8 weeks Consults: Optho, Uro, OBGYN
Pemphigus Vulgaris & Bullous Pemphigoid
Dr. Martinez,MD PV: More common Pemphigussssss is SSSSuperficial Age Range 40-60yo Autoimmune Dz; Ab to DSG 3&1+Nik sign; Flaccid bullae clinically, mucus membrane involvement <10% TBSA TxT: systemic steroids and rituximab IV; 2nd line: Dapsone, Mycophenolate and IVIG. Non-adhesive dressing application BP: Pemphigoidddd is NOT Superficial Disease of elderly F>M 1.3-1autoimmune disorder vs. basement membraneTense blisters clinically; pruritic, tense bullaePruritus is more apparent clinicallyTxt: Topical steroids preferred; IVIG can be used as well per derm’s recs.
Stress & Burnout:
Dr. Huecker, MD Stress= perception of perceived threat. if perceived as negative, research says that this can have negative impacts on healthif perceived as positive=can have beneficial effects on personal potential Stress can impede performance, determined by the individual’s “appraisal” of the situation. Hormesis: phenomena of dose response relationships and over prolonged periods of time can have strengthening effects. Dose of poison a day will make us better. Connect with people daily: compassion does to deplete resourcesOptions to cope: exercise, therapeutic writing, gratitude recognition, thousands available
Necrotizing Fasciitis: Dr. Lehnig, MD Diagnosis: Surgical Exploration CT 90% vs. MRI 86% sensitivityTreatment: “Early Surgical Debridement” Antibiotic Regimen: carbapenam or Zosyn +Vanc, dapto, or linezolid +clindamycin for antitoxin effects
Staphylococcal Scalded Skin Syndrome (SSSS): Dr. Edwards, MD Mostly less than 5 yo; if in adults typically immunocompromised Clinical Exam: +Nikolsky’s sign and will spare mucosal surfaces; + fever typically Diagnosis: Clinical Exam; look for other infections that precipitated the infection. Treatment and Disposition: Typically burn unit admission, Antibiotic Regimen: Typically MSSA but if there are risk factors for MRSA use coverage for MRSA.
EMTALA : Dr. Royalty, MD
Emergency Medical Treatment and Active Labor Act#1: Medical Screening Exam (Everyone gets this no questions asked)#2: If you ID an emergency condition, you must treat and stabilize this, if hospital can’t manage, must get accepting physician to transfer to higher level of care#3: If OSF needs to transfer patient because of lack of ability to care for patient, facility is required to accept patient despite ability to pay, etc. Transfers: All pertinent records and imaging should accompany patient or be sent electronically ASAP.
Decisional Capacity: Dr. Yff, MD Informed Consent: understand treatment, potential risks and benefits, and reasonable alternatives
4 Components: relevant info, appreciation of consequences (insight), reasoning of choice & communicating a choice. Estimated, 48% of patients hospitalized are not capable of making decisions in a hospital setting MacCAT-T: decisional tool to evaluate capacity.
Treatment of Non-Emergent Hyperglycemia in the ED: Sue McGowan, APRN Diagnosis: Glucose >126 fasting, a1c over 6.5%, and Random BG >200 + symptoms Targets for Diabetes: Premeal BG 80-130, post prandial <180, a1c <7Treatment: Diet and exercise-> Metformin if renal function adequate and no GI intolerance (500mg BID)-> a1c 8.5% (ADA recommends 2nd agent-> a1c 9% (see ADA guidelines)-> a1c Long Acting: 24 hour coverage “peak less”; glargine,basaglar, detemir, degludec (each vial has 30 days 300U)NPH/Intermed acting: onset 1-3 and peak 6-12 hours (NPH and 70:30 insulin very cheap) Rapid Acting: 5-10 min onset peaks1-2 hours (the “logs” and apidra and fiaspInitiating Insulin: basal or NPH 10U/day or 0.1-0.2 U/kg/day goal <130 before breakfast (titrate ever 3 days by increasing 2 U to hit morning goal)Glucose tabs=fastest method to correct hypoglycemia OOH (OTC and cheap)Send prescription for glucagon for 2ndary person to admin for rescue. Diabetes Supplies: glucometer, test strips, lancets, and needles for insulin. Diabetic NP: 10am-6:30pm ULH consult via cerner.
Electrical Injuries: Dr. Leavitt, MD Low voltage <600V (most household circuits around 120V)High Voltage 600V<Peds: chewing on electrical cords, must admit these, delayed necrosis of S. labial A. Lighting Injuries: Initiate CPR immediately if pulseless; ruptured TMs, A/C worse than D/C injuries
Check out this very brief Amal Mattu article about that pesky ECG after ROSC. Bottom line: Wait at least 8 minutes to obtain the ECG if you obtain ROSC. This isn’t that wild of an idea, and often it takes a good 10 minutes to set up the machine and stop doing your other resus tasks. But don’t be compelled to get the ECG as fast as possible, as the delay of 8 minutes can reduce false + STEMI. Check out this long article he cites.
![Room9er ["Room Niner"]:](https://room9er.com/wp-content/uploads/2020/03/cropped-Screen-Shot-2020-03-08-at-3.16.16-PM.png)