Heparin à no renal metabolism (helpful in patients with renal failure)
Thrombocytopenia, HIT, heparin resistance, hyperkalemia from aldosterone suppression
Half-life 30-60 minutes, immediate onset
IV administration for VTE, must be administered inpatient
Careful monitoring required
Enoxaparin (Lovenox, LMWH)
Derived from heparin
3-5 hour onset, no monitoring required, patients may self-administer
Similar outcomes compared to heparin with regards to recurrent VTEs, some data suggest lower bleeding risk
Renal clearance, avoid in renal dysfunction
Similar precautions as heparin
Lower incidence of HIT, but still contraindicated in patients with HIT
Subcutaneous dose for VTE
Apixaban (Eliquis)
Factor Xa inhibitor
Half-life 9-14 hours, BID dosing
Renal clearance, caution in renal insufficiency
Rivaroxaban (Xarelto)
Factor Xa inhibitor
Half-life 5-19 hours, daily dosing
Must be taken with food to be effective
Renal clearance, caution in renal insufficiency
Dabigatran (Pradaxa)
Direct thrombin inhibitor
Half-life 12-14 hours
VTE dosing after 5 days of bridging, BID dosing
2020 AHS Guidelines on Management of VTE suggests using DOACs over Warfarin
Does not apply to all patients
AMPLIFY à Eliquis non-inferior to standard therapy (Warfarin, LMWH), less bleeding complications
EINSTEIN DVT/PE à Xarelto non-inferior to standard therapy
Does not recommend one DOAC vs. another, recommend using patient specific factors to guide clinical decision making
Recommends home treatment for patients with uncomplicated DVT
2020 AHS guidelines recommend considering home treatment for patients with low-risk PE (PESI Score risk stratification), conditional recommendation
Extremely important to counsel patients when being discharged on these high-risk medications, ensue follow-up and understanding of risks and return precautions
Pneumomediastinum (Dr. Alia)
Presence of free air in the mediastinum
Spontaneous (idiopathic, tobacco use, recreational drug use) vs. secondary (i.e. traumatic, iatrogenic) etiologies
30% have normal chest x-rays à CT Chest is preferred diagnostic modality
“Continuous diaphragm sign” on XR
Management:
Treat underlying cause
Supportive care à typically resolves spontaneously in 1-2 weeks
Disposition:
Primary à discharge with PCP follow-up
Secondary à management of underlying cause, typically will require admission
Lung Abscess, Parapneumonic Effusion, Empyema or (Dr. Edwards)
Typically polymicrobial, affected tissue at risk for necrosis and cavitation
Diagnosed via CXR vs. CT Chest (also recommended following XR diagnosis)
Ultrasound helpful for evaluation of effusions and for procedure guidance
Obtain blood and sputum cultures (blood cultures frequently negative in empyema)
Treatment à empiric antibiotics with anaerobic coverage
Empyema, effusions require drainage
VATS for complicated effusions and empyema
Thoracentesis provides definitive diagnosis for empyema (distinguishes between effusion and empyema) à body fluid cultures and diagnostics must be obtained
Pneumonia for EM Residents (Dr. Eisenstat)
CAP à everything not HAP or VAP
HAP à >48 hours from time of admission, previous admission within 90 days
Cover for pseudomonas and MRSA
VAP à >48 of intubation time, recent previous intubation
Cover for pseudomonas and MRSA
Therapy tailored based on sensitivities and culture results
Normal vital signs and normal respiratory examination have good negative predictive value in most patients
Procalcitonin à good predictor of blood culture positivity
Hypoglycemia, lactate à predictors of 28-30 day mortality
2-view chest XR recommended
Flu test patients with CAP during flu season
Give antibiotics to all patients clinically suspected to have CAP regardless of procalcitonin
Clinical judgement + decision tool is best (PSI > CURB-65)
Healthy, outpatient à amoxicillin vs. doxycycline vs. macrolide (if local resistance is <25%)
Comorbidities, outpatient à Augmentin vs. cephalosporin (cefpodoxime, cefuroxime) AND macrolide vs. doxycycline
Monotherapy with respiratory fluoroquinolone also acceptable, but consider risk factors
Inpatient treatment of CAP in adults without risk factors for MRSA or Pseudomonas
Combination therapy with Beta-lactam + macrolide or doxycycline
Coverage of anaerobic pathogens not necessary in admitted patients who are suspected to have aspiration PNA
Inpatient treatment of patients with risk factors for MRSA and Pseudomonas à vancomycin or linezolid for MRSA, Zosyn/cefepime/meropenem for Pseudomonas
Corticosteroids are unnecessary unless used in patients persistently hypotensive despite IVF and vasopressors (i.e. surviving sepsis guidelines) but evidence is not conclusive
Give Tamiflu to patients with CPA who test positive for flu (regardless of inpatient vs. outpatient or duration of symptoms), give antibiotics regardless of flu positivity
Antibiotic treatment duration for outpatient treatment of CAP à 5-7 days
No follow-up CXR necessary in adults who are improving following treatment
Assess hydration status (tears, saliva, capillary refill, wet diapers in 24 hours)
Check the ears (occasionally have coinfections)
Always do an abdominal examination to assess for hepatosplenomegaly
Management:
Suction! Suction! Suction!
CXR unnecessary unless concern for superinfection or clinical picture not consistent with typical bronchiolitis (prolonged symptoms, high fevers, persistent hypoxia) à atelectasis and peribronchial cuffing on CXR if obtained
Viral testing is not always necessary (exception: influenza, COVID-19, RSV <1 month causes apnea)
Respiratory support
Dexamethasone in patients <1yo with no history of wheezing did not demonstrate benefit
Albuterol has not been shown to benefit patients
Bronchiolitis Score is helpful with risk stratification
Discharge Criteria
O2 saturation >90% while awake
Adequate PO intake
Mild/moderate work of breathing
Reliable caretaker
Timely pediatrician follow-up in 1-2 days
Admission Criteria
Hypoxemia
Severe respiratory distress
Apnea
High-risk patients
Poor oral intake
Parents uncomfortable with discharge
Consider intubation if…
Recurrent apnea
Declining mental status
Not improving with respiratory support
Asthma Exacerbation
Antibody binds antigen à release of histamine/leukotrienes à inflammation à bronchospasm
Pediatric Respiratory Assessment Measure (PRAM) is helpful for risk stratification
Timing of medications is key!
CXR is not required unless concern for complicating factors
Management:
Beta-2 agonists
Albuterol à MDI vs. nebulizer
Always use a spacer!
Short vs. 1-hour long vs. continuous albuterol nebulizer
Discharge à take 4 puffs every 4 hours for the next 48 hours, then as needed after that
Remember to write for MDI with spacer if discharging with albuterol prescription
Terbutaline à IV vs. SQ
Corticosteroids à mainstay of treatment considering the pathophysiology
Dexamethasone
Prednisone/prednisolone
Methylprednisolone
Ipratropium nebulizer
Anticholinergic
Often used in conjunction with albuterol nebulizer
Magnesium sulfate
Smooth-muscle relaxer
Can cause smooth-muscle relaxation in the vasculature à hypotension (consider IVF bolus)
Epinephrine à anaphylaxis dosing
Admission Criteria
Requiring >1 1-hour long albuterol
Respiratory distress
Hypoxemia (O2 <92%)
Dehydration
Croup (laryngotracheobronchitis à upper airway)
Acute subglottic inflammation
Morbidity is greatest in 1st year of life due to narrower subglottic airway
Affects children aged 6-36 months
Classically caused by parainfluenza virus, but also caused by many other viruses
Clinical presentation:
Barky cough
Inspiratory stridor (more concerning if occurring at rest)
Tachypnea
Suprasternal retractions (hypoxia, intercostal retractions, abnormal breath sounds, subcostal retractions are uncommon à croup is a disease of the upper airway, if hypoxia is present and lungs are clear to auscultation there should be high concern for impending upper airway compromise)
Low-grade fever
Management
Dexamethasone
Racemic epinephrine for resting stridor or respiratory distress (can repeat every 15-20 minutes)
Monitor for 3-4 hours prior to discharge if administering racemic epinephrine à admit for refractory stridor or if repeat dosing of racemic epinephrine is required
Consider Heliox for severe respiratory distress as it decreases turbulent flow
Documentation Lecture (Ashley Chesman)
Critical Care Documentation
7.2% of all ED visits reported to Medicare in 2019 were reported as critical care
Time at bedside, but also time spent engaged in work directly related to the patient’s care:
Reviewing test results and imaging studies
Consulting services
Placing orders
Procedures billed separately
Billings starts at 30 minutes à critical care time requests <30 minutes may not be compensated
E/M and Critical Care Same Date of Service
Can now bill for E/M and Critical Care on the same date/visit
Documentation must support decompensation to a state requiring critical care
Remember to document critical care time beginning in residency!
Subclavian Central Venous Lines (Drs. Nichols and Leavitt)
Contraindications
Overlying infection
Anatomic obstruction
Fracture of ipsilateral clavicle
Relative à coagulopathy (harder to compress and apply pressure to the subclavian site)
Complications
Arterial injury
Pneumothorax
Air embolism
Cardiac dysrhythmia
Infection
Bleeding
Supra- vs. Infraclavicular Subclavian Access
Infraclavicular
Utilizes short-axis ultrasound
Index finger on the sternal notch and thumb at the midpoint of the clavicle at the angle
Make contact with the clavicle and “walk-down” and pass under the clavicle vs. insert needle further laterally to avoid having to “walk-down” the clavicle
Ultrasound assisted technique utilizes short-axis
Supraclavicular
Well-defined landmarks (claviculo-SCM angle)
1 cm superior and 1 cm lateral to the claviculo-SCM angle
5-15 degrees above the coronal plane
Don’t advance past 3 cm
Ultrasound assisted technique utilizes long-axis as opposed to the short-axes
Shorter distance from skin to vein
Larger target area
Straighter path to the SVC
Less proximity to the lung
Fewer complications compared to infraclavicular
Found to be non-inferior to the infraclavicular approach
Lightning Lectures – Pulmonary Cases (Drs. Bishop and Slaven)
Tuberculosis
TB concern à NAAT + sputum cultures to assist with diagnosis (95% sensitive)
Negative pressure room with airborne precautions, PPE precautions for providers, HIV test if TB suspected
Mycobacterium tuberculosis à aerobic rod, highly antigenic à can disseminate systemically if initial granuloma formation fails to contain the infection
Immunocompromised population at highest risk (2x)
bCG vaccine recipients all have positive TB skin tests (PPD)
Interferon test does not distinguish between latent and active TB
Active TB àINH, RIF, pyrizanimide, ethambutol x8 weeks à INH/RIF x18 weeks + B6
Hepatotoxicity
Latent TB à INH x9 months + B6
Must contact Public Health Department prior to discharge
Spontaneous Pneumothorax
Sudden pleuritic chest pain, increased work of breathing, hypoxia
DDx with examination + upright CXR
CT chest is very sensitive/specific but takes time to obtain
Consider US
Management:
Supplemental O2
Unstable à Decompression (treatment for tension PTX)
Stable, small à consider observation 4-6 hours, repeat CXR, must ensure follow-up within 24 hours à admit any recurrent or complicated PTX
Admit everything else and all PTX caused by comorbidities
Inhaled Intoxicants (Dr. Eisenstat)
Huffing/bagging à toluene is intoxicating substance (higher in gold and silver paints)
Can cause NAGMA, renal tubular acidosis, hypokalemia, chronic encephalopathy
Sudden sniffing death syndrome à hydrocarbon (huffing) + high levels of catecholamine surge à death
Generally not recommended to use epinephrine/norepinephrine in patients suspected of hydrocarbon toxicity
Aluminum encephalopathy from black tar heroin use à basal ganglia lesions on MRI
High water solubility à chlorine, tear gases, ammonia (mucous membrane effects)
Low water solubility à phosgene, chloramine, nitrogen dioxide (delayed pulmonary edema)
Phosphine gas/aluminum phosphide à occurs when aluminum phosphide interacts with moisture à can expose providers during ventilation efforts/resuscitation
Nitrogen dioxide à silo fillers
Phosgene à choking agent, delayed pulmonary edema
Tear gases à OC spray AKA pepper spray AKA mace à capsaicin-based tear gas à causes severe burning and irritation, CS (military grade) is more potent
Treatment is irritation (consider Morgan lens for eye involvement)
Organophosphates à nerve agents àdecontamination, atropine, pralidoxime, supportive care
Asphyxiants à methane, propane, argon gas à sudden collapse, helper also collapses, etc.
Carbon monoxide à can be high in smokers (COHgb of 10) and large cities
Treatment is controversial à begins with O2 therapy (100% FiO2, NRBM)
Consider hyperbaric in COHgb levels >25 (15 in pregnant patients due to fetal Hgb affinity for CO) or signs of organ dysfunction (AMS, NSTEMI)
The reason for HBO therapy is to reduce long-term symptoms, which are often delayed (up to 6-8 weeks), not life-saving
Cyanide à combustion of nitriles in house fires à leads to unconsciousness and CV collapse à elevated lactate (>8 with ingestion, >10 in house fires) with high suspicion
Amyl nitrite (induces methemoglobinemia) vs. Hydroxocobalamin/Cyanokit (safer, colors urine organe/red) with levels >8
Hydrogen sulfide à cellular asphyxiant similar to cyanide à rotten-egg smell in low concentrations (odorless in high concentrations), used in chemical suicide
COPD and Asthma Cases (Dr. French)
COPD à titrate goal O2 to 88-92%
Patients need PPV
Antibiotics for COPD exacerbation à some evidence for reduced rate of readmission/representation
Remember to consider breath-stacking/auto-PEEP in MV
PRAM Score for asthma exacerbation à follow-up 3 hours with additional PRAM Score, can assist with disposition planning
PRAM >12 à marker of impending respiratory failure
ED Management of Brain Aneurisms (Dr. Ding)
Unstable à repair
Stable à timely outpatient follow-up
1/3 will die, 1/3 will be self-sufficient at discharge, 1/3 will have poor recovery
Surgery (clip) vs. endovascular (coiling)
Treatment modality depends on multiple factors à age, medical comorbidities, multiple aneurisms, location, size, symptoms
Which aneurisms will rupture à location (anterior communicating, posterior communicating aa. higher risk) vs. size of aneurism vs. risk factors vs. family history vs. connective tissue disease/AAA vs. stress vs. growth of aneurism
Enlarging and symptomatic unruptured aneurisms should be treated
Before/after stent-coiling or flow diversion à DAPT
Consult NES for incidentally found aneurisms on imaging, both admitted and discharged
CTA/MRA for history of aneurism and symptoms
Consider SAH in post-coital headache
Don’t forget about LP vs. MRI in patients suspicious for SAH with negative CT/CTA
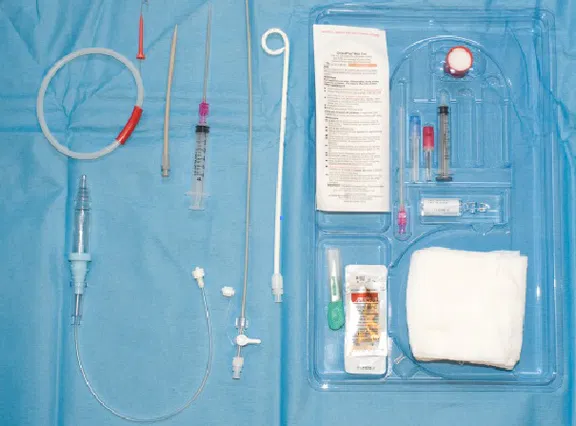
Large-bore chest tubes are still recommended for more viscous effusions such as empyema or hemothorax
Step-by-step Guide:
Prepare the chest tube atrium and ensure appropriate length tubing is available for low wall suctioning once the procedure is complete
Place the patient in either a lateral recumbent or supine body position with the head of the bed elevated to 30-45 degrees, or in a seated position with the patient leaning slightly forward for posterior tube placement (i.e. tube placement for drainage of pleural effusions, ultrasound guidance is recommended for posterior tube placement similar to with thoracentesis both to identify the location of the effusion and due to the increased presence of vascular structures between the rib spaces posteriorly)
Identify the location of insertion, usually the 4-5th intercostal space at the mid-axillary line (similar to large-bore chest tube placement) at the level of the nipple. Remember the “safety triangle” bordered by the lateral edges of the pectoralis and latissimus dorsi muscles where there is a decreased risk for damage to underlying vascular, nervous, and organ structures
Sterilize the skin surrounding the site of insertion and drape the patient accordingly using the drape provided in the kit, or by using sterile towels if preferred (remember to leave the nipple exposed to assist with identifying landmarks during catheter placement)
Measure the small-bore catheter in front of the patient’s chest to determine the appropriate depth of insertion in a manner which ensures placement towards to superior aspect of the chest with all side ports within the pleural cavity (remember, the catheter can be withdrawn but not inserted further once the procedure is complete, similar to placing a central venous catheter)
Generously anesthetize the skin at the desired site of insertion, advancing your needle deeper over the superior aspect of the rib to minimize the risk of damage to the neurovascular bundle, withdrawing prior to injecting lidocaine as the needle progresses through the soft tissue. Be sure to anesthetize the parietal pleural during this process, as it is fine for the needle tip to pass into the chest cavity
Gently advance the finder needle over the superior aspect of the rib through the intercostal musculature similarly to the previous step while steadily drawing back against the syringe plunger as the needle tip advances. The plunger pressure will give way once access into the pleural cavity is achieved. Consider loading the finder needle syringe with several mL of sterile water for visualization of air bubbles in the syringe to assist with this step
Once access to the pleural space has been achieved remove the syringe from the finder needle and insert the guide wire into the back of the finder needle passing the wire into the pleural cavity in such a manner that leaves most of the wire hanging outside of the patient
Remove the needle from the patient and make a small incision in the skin at the base of the guide wire using the provided 11-blade scalpel
Pass the dilator over the guidewire and into the pleural space feeling it give-way once it has pierced the parietal pleura and entered the thoracic cavity. Be sure to visualize the guide wire exiting the back of the dilator prior to insertion to ensure the wire is not accidentally lost within the chest. The dilator may be removed once this step is complete
Pass the small-bore catheter within its trocar over the guide wire and into the pleural space in a manner that ensures all side ports are within the space. Generally, the first black indicator line can be used for small and thin patients, the second black line for the average adult, and the third black line for large adults. Similarly to the above step, ensure the guide wire is visualized exiting the back of the trocar prior to insertion.
![Room9er ["Room Niner"]:](https://room9er.com/wp-content/uploads/2020/03/cropped-Screen-Shot-2020-03-08-at-3.16.16-PM.png)