Hey guys, I was hoping to get your input on an interesting case I had at Kosair over the weekend.
16 yo F (6 ft, 150 lb…so basically an adult) with a PMH of depression, self injury, and prior suicide attempt presents after ingesting citalopram 40 mg x 90 pills (her prescription, just filled 2 days ago) and concerta 10 mg x 8-9 pills (her brother’s). Patient had been at a party the night before, admitted to EtOH. Parents found out about the party the morning of admission and they had a big fight, took away car keys, etc. Patient decides to retaliate by swallowing pills, doesn’t tell anyone. Parents find her altered about 10:30, at Kosair at 11:40. Best guess is ingestion occurred sometime around 9-9:30am. Had one seizure at home per family, and one en route per EMS. Generalized, tonic-clonic, brief.
Initial exam shows a drowsy but arousable patient. Answers orientation questions x3. Initial vitals show HR 147, BP 135/70, RR 25, 93% on some oxygen (can’t remember if NC or nonrebreather). Patient denies CP, palpitations, SOB, abd pain, N/V, weakness/numbness. 4mm, PERRL. MAE equally. Old self injury scars noted on wrists bilaterally. Exam otherwise unremarkable.
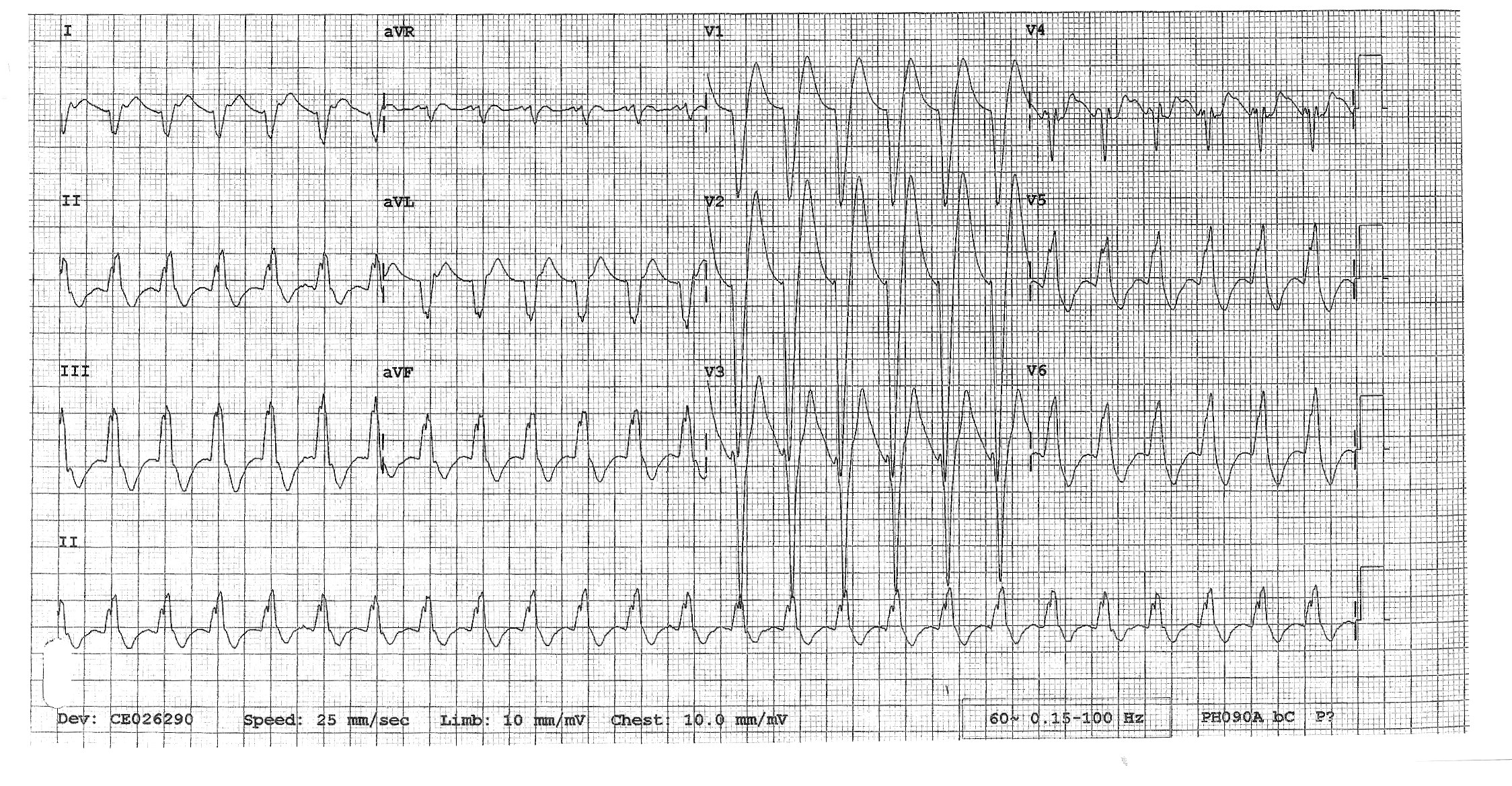
We start IVs, get her on a non-rebreather, get IV fluids going. Agree that charcoal seems like a bad idea with her mental status and seizures. Mom has shown up, and as we’re getting some additional history from her, respiratory is placing EKG leads. I’ve talked to poison control. Then, about 20 minutes into her stay, she seizes again. We bag her through the seizure, again generalized tonic-clonic, and just as we’re pushing 2 mg of IV Ativan she comes out of it. She appears post-ictal, but is maintaining her airway. We load her with Keppra, and as I glance at the monitor behind the attending’s head, I notice that her rhythm has changed and she looks like she’s got a wide QRS. We confirm she still has good pulses, still out of it mentally, and since she’s already connected to the EKG leads we grab one (time stamp 12:04):
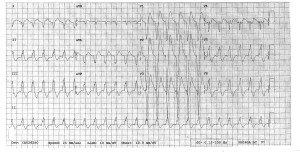
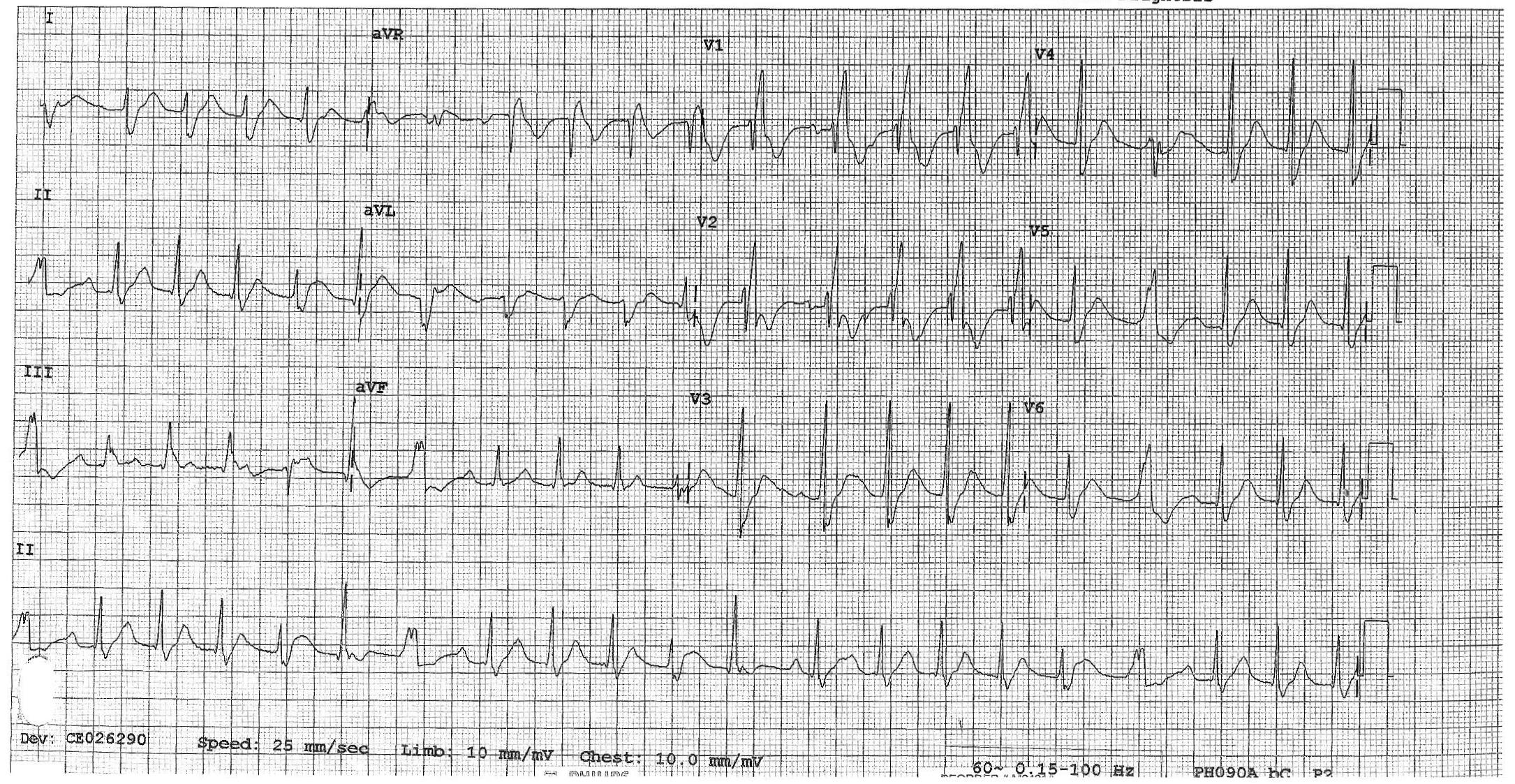
By the time we get this printed off (!!!!) she appears to have spontaneously converted back to sinus on the monitor. But woah, holy wide QRS/long QT batman! As the attending and I are pouring over the first EKG we get another one immediately (time stamp 12:08):
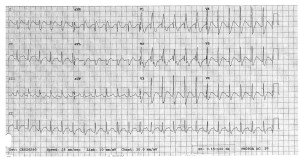
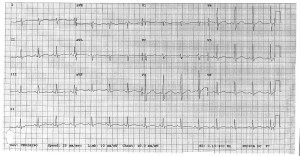
Thankfully, the QRS appears to have normalized, but we’ve still got a loooong QT, one of the things poison control definitely told us to look out for. Having seen a few similar ingestions at University, I suggest it’s time for bicarb. The attending wants to confirm and we quickly call poison control back, they agree and suggest starting a bicarb gtt, with pH goal of 7.45-7.55. Now we look back at the monitor and she’s throwing a ton of PVCs, captured here on EKG #3 (time stamp 12:12):

At this point, we opt to push an amp of bicarb while we’re waiting for pharmacy to tube up the bicarb gtt. I have to say, we see it start to work pretty darn quickly. The PVCs slow down, and her rate really starts to head back towards normal. We get an iStat (shot me down when I suggested one earlier), and a few minutes after we’ve pushed the bicarb we get an initial pH of 7.15, pCO2 of 51.5, HCO3 of 18, BE -11, and AG of 21. Electrolytes were WNL. By this time we also know her pregnancy is negative, and her serum tox is negative, no acetaminophen/salicylates on board. At this point, we talk about intubation as the patient’s mental status is still waxing/waning and she’s breathing shallowly with brief periods of apnea, almost like an opiate overdose. Attending wants to hold off, so I go off to call the PICU resident…and end up having to hang up the conversation halfway through when he changes his mind.
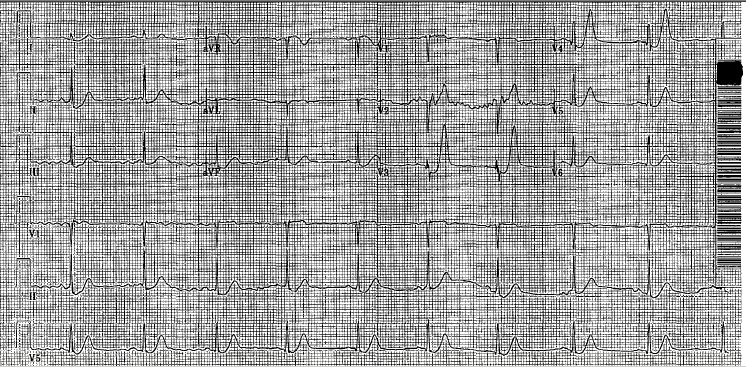
So we intubate her (finally got a peds tube…in an adult), the bicarb gtt comes up from pharmacy, they’re cleaning the PICU bed her, the last EKG looks 1000x better, and all’s well that ends well (time stamp 13:08):
So I’m curious to see what your all’s suggestions/thoughts are on this case. Looking back at that first EKG, how would you classify it? We’ve got a wide complex, monomorphic tachycardia that to me looks like sustained V tach (with a pulse). The long QT doesn’t surprise me, but this rhythm does as you’d typically you’d worry about it devolving into Torsades, but that’s not what this is.
Looking back, things I would have done differently: get a temperature sooner/order a total CK (serotonin syndrome could have been a factor and we don’t have a recorded temp until she’d almost 2 hours into her stay, no one ever ordered a CK), intubate sooner, loading her with keppra when she hit the door after 2 witnessed seizures, maybe could have prevented the 3rd?
Also, if you’re curious, I found this “Toxicology Conundrum” on LITFL that specifically discusses citalopram overdose. Has some good info, citalopram is definitely one of the more potent SSRIs, and QT prolongation is dose dependent and can be seen after ingesting >600 mg (this chick took 3.6 GRAMS). Seizures are also fairly rare, only seen in 2-3% of cases.
![Room9er ["Room Niner"]:](https://room9er.com/wp-content/uploads/2020/03/cropped-Screen-Shot-2020-03-08-at-3.16.16-PM.png)