![Room9er ["Room Niner"]:](https://room9er.com/wp-content/uploads/2020/03/cropped-Screen-Shot-2020-03-08-at-3.16.16-PM.png)
Previously healthy, middle aged male; presenting to room 9 via ground EMS.
Unrestrained single-occupant, rollover MVA. Pt found “partially ejected” through the sunroof of the car.
Awake and oriented with EMS. Hemodynamically stable en route to the hospital. EMS report called and patient room 9ed by the mechanism.
Patient arrives on a backboard and c-collared. He is awake and oriented, GCS 15. ABCs intact. Vital signs all normal.
Exam significant for abrasion/contusion to the R central forehead (skin otherwise intact), bilateral wrist tenderness without deformity.

Photo 1; Photographed with patient permission specifically for academic posting
Chest, abdomen, pelvis without acute traumatic findings.
And… weakness in all extremities; upper worse than lower; distal much worse than proximal. He actually has pretty well-maintained movement about the shoulders but his forearms, hands, wrist fling wildly and uncontrolled.
Motor exam:
Delt Bi Tri WrFl WrExt Grip
RUE: 5 4 2 1 1 1
LUE: 5 4 2 1 1 1
HipFl HipExt KnFl KnExt DorsiF PlantF
RLE: 4 4 3 3 2 2
LLE: 4 4 3 3 2 2
The diagnosis is probably already fairly certain at this point (if not read along).
CT man-scan is obtained by mechanism.
Sagittal CT scan

Still image from CT scan. Demonstrating congenital fusion of C2 and C3 (Klippel-Feil syndrome). There is congenital narrowing of the spinal canal. There are multilevel degenerative changes. There is an avulsion fracture of the anterior-inferior “tip” of the C5 vertebral body. THIS “teardrop” avulsion fracture is associated with extension injury (also evidenced by the forehead abrasion/contusion).
Neurosurgery had already been consulted. The MRI of the cervical spine was ordered and pending.
A Foley catheter was placed for urinary retention.

“IMPRESSION: 1. Posterior disc osteophyte complexes at C4-C5 and C5-C6 in conjunction with a diffusely congenitally narrowed spinal canal cause severe spinal canal stenosis and mass effect on the underlying spinal cord which shows signal abnormality consistent with contusion/edema, possibly superimposed upon myelomalacia.2. Redemonstrated acute mildly displaced fracture along the anterior aspect of the C5 lower endplate. Possible C5 vertebral body bony contusion noted. Associated mild anterior paraspinal edema. Small amount of heterogeneous T1 signal posterior to the C5 and C6 vertebral bodies may represent a combination of blood products, edema, and disc material.3. Mild increased STIR signal intensity within the interspinous spaces from C3 through C7, which could indicate interspinous ligament sprain injury”
The patient was taken to the operative room with neurosurgery for spinal cord decompression. He was maintained on pressors to maintain high MAPs (>85mmHg).
At the time of hospital discharge, he had regained some function including wrist flexion and extension (although still weak), plantar and dorsiflexion returning. He was discharged to rehab.
CENTRAL CORD SYNDROME
As the name implied Central Cord Syndrome is an incomplete spinal cord injury.
Of the incomplete syndromes, it is the most common.
Most commonly occurring in hyperextension injuries of the neck.
Mostly in those with pre-existing degenerative disease of the cervical spine.
The classic presentation of upper limb weakness >> lower limb weakness. Distal >> proximal motor loss.
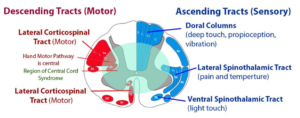
Variable sensory loss of primarily pain and temperature.
Urinary retention!! (place a foley catheter early!)
Some require neurosurgical intervention (worsening exam, acute cord compression (herniated disk), or have unstable fractures of the cervical spine)
Admit to ICU for neuro-checks.
Key words: Central cord syndrome, spinal cord injury, neurosurgery, trauma