![Room9er ["Room Niner"]:](https://room9er.com/wp-content/uploads/2020/03/cropped-Screen-Shot-2020-03-08-at-3.16.16-PM.png)
Hey all,
I got the privilege of going to ACEP last week in Boston. When I got the schedule one of the lectures that stood out to be was a PE lecture by Jeffrey Kline. Some of you may recognize the name but if not, he is an attending at IU with a special interest in thromboembolism. He is very active on twitter at @klinelab and wrote the Thromboembolism chapter in Tintinalli’s. After talking about PE last month and specifically approach to PE in the pregnant patient, I thought a summary of the key points would make for a worthwhile post.
The first question in the discussion of VTE should be ‘who actually needs to be tested?’ If someone comes in complaining of recent chest pain or dyspnea, PE needs to be included in the differential. If they are not complaining of those recently and have normal vitals (at all times) then you don’t need to go chasing down a clot that isn’t there. If the patient does complain of those then some sort of documentation is required to show you considered a PE. Even stating ‘I think PE is unlikely because of X, Y and Z’ would likely be enough. Now if your pretest probability is anything other than very low, some combination of wells, perc, Geneva should be applied. I like the following algorithm which I think Kline discussed on EMRap towards the end of last year.
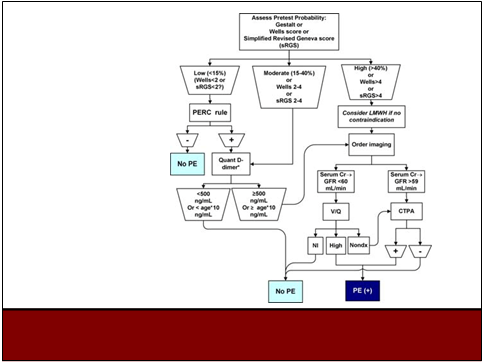
Following that algorithm helps cut down on the number of ct scans you’ll order, cuts down your false-positives, radiation exposure, and contrast induced nephropathy without increasing the number of significant PE’s that you miss.
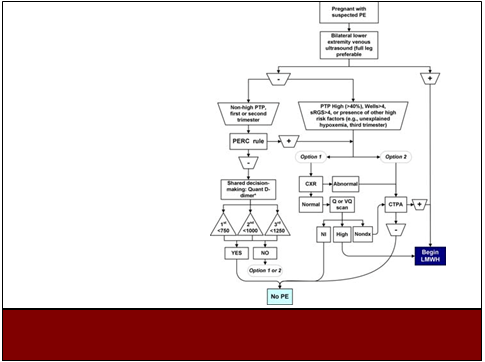
As far as the pregnant patient, I think everyone knows to start with the lower extremity ultrasounds in hopes of an answer that would let you initiate treatment. However, when that is inevitably negative, there is also an algorithm for that scenario that incorporates a trimester adjusted d dimer.
The other main takeaway from this talk was the disposition change on some of the low risk patients. Dr. Kline said he has sent about 70 patients home from the ED after being diagnosed with PE. To stratify who falls into low risk, you can apply the sPESI or HESTIA score as well as who is at low risk of bleeding.
–Simplified PESI-if any +, pt is NOT low risk:
age greater than 80
history of cancer
history of chronic cardiopulmonary disease
pulse greater than 100
BP less than 100
O2 sat less than 90
–Hestia-pt CAN BE considered low risk if
BP greater than 100
No thrombolysis needed
No active bleeding
02 sats greater than 90
Not already anticoagulated
No other medical or social reason for admission
Cr clearance greater than 30
not pregnant, no severe liver disease
For these people they’ll initiate rivaroxaban or apixaban in the ED and send them home with a prescription. The only failures they’ve experienced are people who returned requiring additional pain management. Has anyone done this or considered it? The majority of our patient population would not satisfy these requirements or, frankly, be reliable enough to consider outpatient management, but what about people working in the community with a different population?
Lastly, we all know to look for S1Q3T3 on the ekg to raise suspicion for PE but the odds ratio is only 2.06. Inverted T’s in V2 and V3 have odds ratios of 6.94 and 7.07 respectively, and are the most SPECIFIC ekg finding in pulmonary embolism