![Room9er ["Room Niner"]:](https://room9er.com/wp-content/uploads/2020/03/cropped-Screen-Shot-2020-03-08-at-3.16.16-PM.png)
58 yo F presents to the ED for cough, chest pain, and fatigue for 1wk. She has sharp, atypical sounding chest pain. But she is 58 and has risk factors: HTN, HLD, 0.5ppd smoker x48yrs. Better get an EKG.
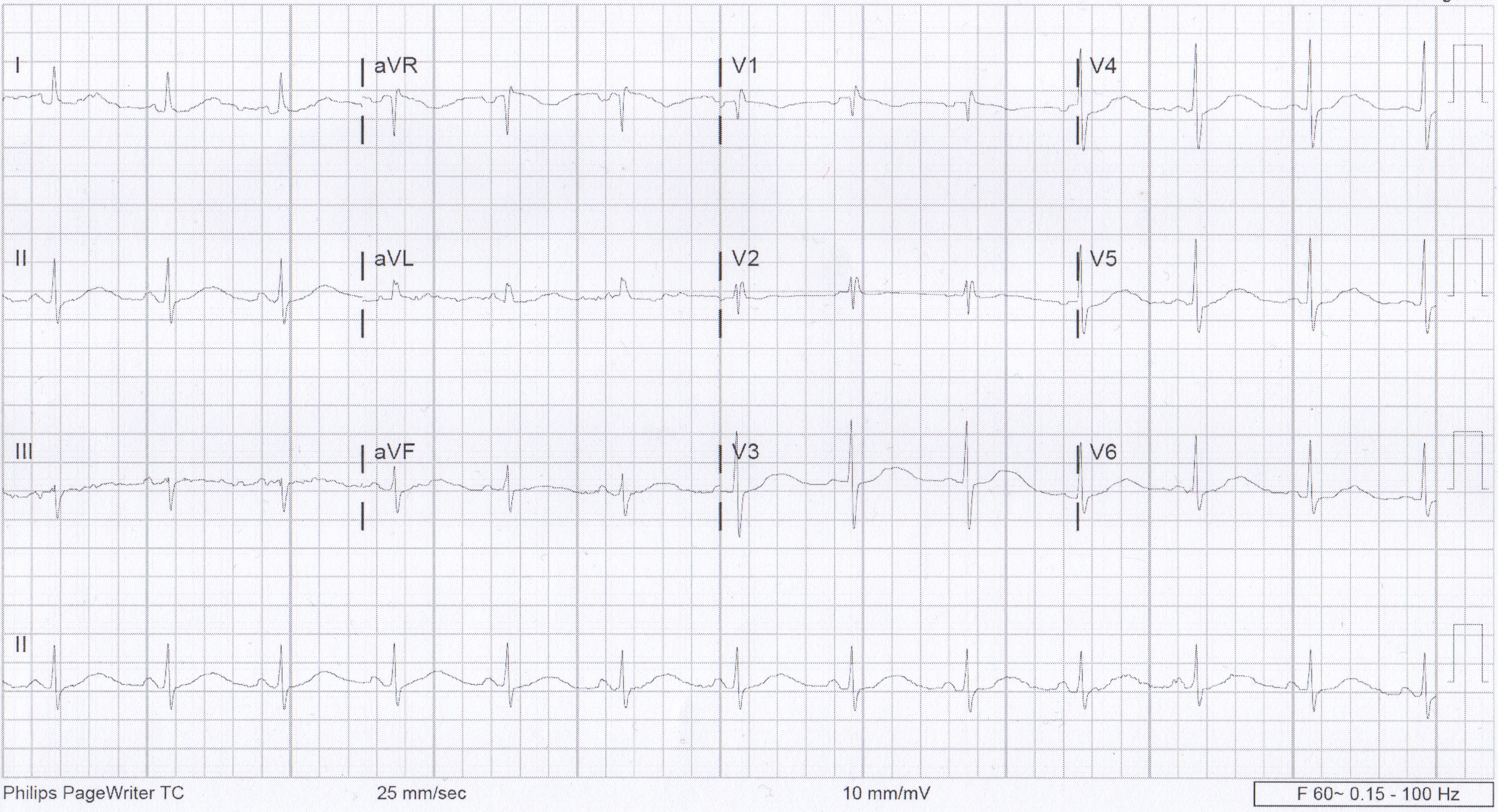
Initial EKG
Awesome, no STEMI. Done with EKG right? Hope you didn’t miss that really long QT interval.
First, how do we measure the QT?
 We usually talk about QTc rather than just the QT. This is because the QT interval varies depending on the HR. Using a correction equation standardizes the interval so it can be interpreted regardless of the HR. The EKG computer does give a calculation of the QTc, because we are obviously not hand calculating this on every patient. You should compare what the computer calculates to your gestalt when you review the EKG. If there are any concerns or discrepancies, you should hand calculate the QTc. MDCalc has an easy to use calculator. Above is the Bazett’s formula, which seems to be the most commonly used. Other formulas do exist. QTc is considered prolonged if > 440ms in men or > 460ms in women.
We usually talk about QTc rather than just the QT. This is because the QT interval varies depending on the HR. Using a correction equation standardizes the interval so it can be interpreted regardless of the HR. The EKG computer does give a calculation of the QTc, because we are obviously not hand calculating this on every patient. You should compare what the computer calculates to your gestalt when you review the EKG. If there are any concerns or discrepancies, you should hand calculate the QTc. MDCalc has an easy to use calculator. Above is the Bazett’s formula, which seems to be the most commonly used. Other formulas do exist. QTc is considered prolonged if > 440ms in men or > 460ms in women.
Next, why do we care?
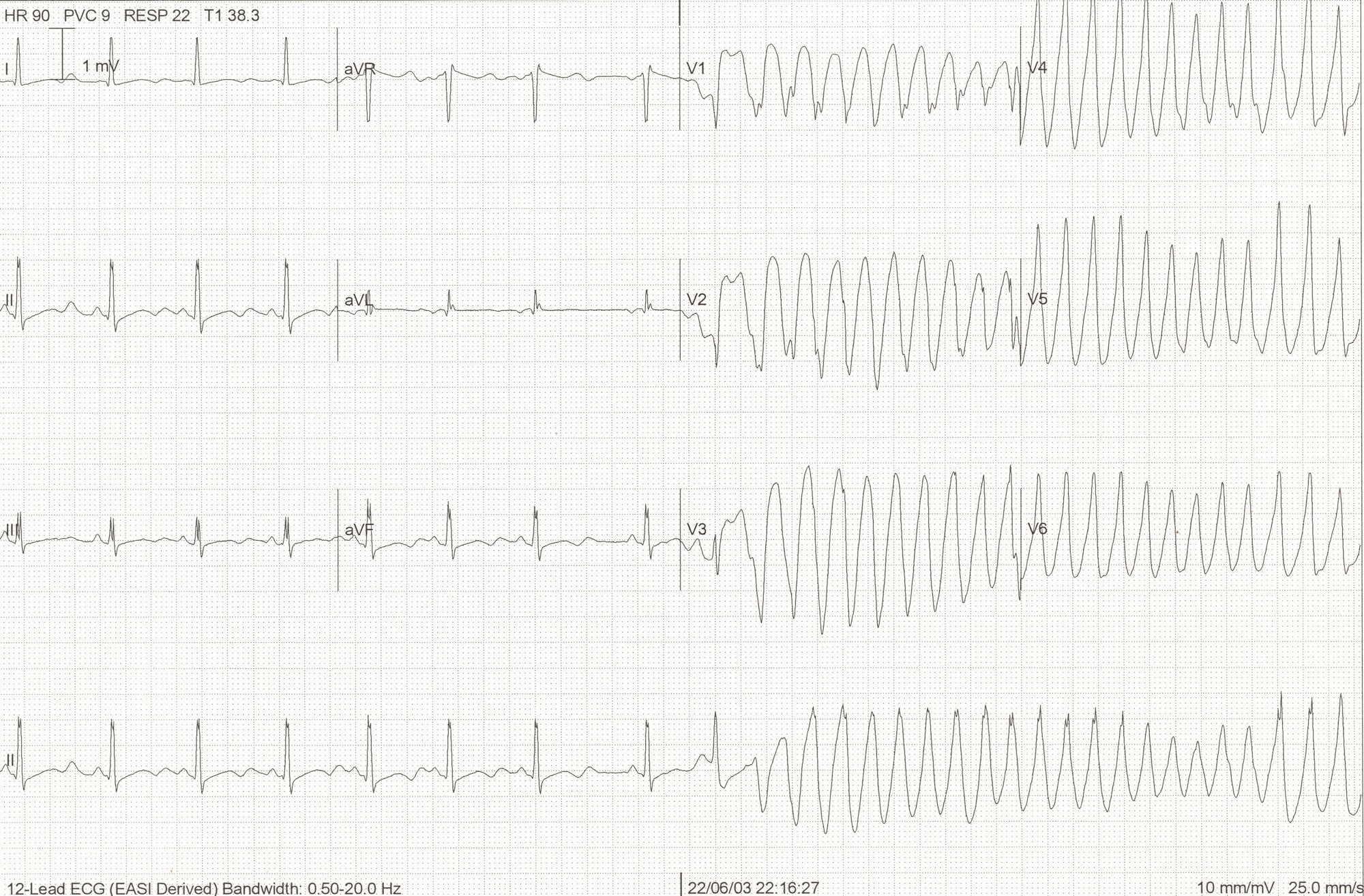
This is the start of Polymorphic VT. There are several things that can cause this rhythm. Long QT is one possible cause. When Polymorphic VT is caused by a prolonged QT we give it a special name, torsades de pointes. The mechanism behind this is demonstrated on the above EKG. As the QT interval becomes more prolonged, there is a higher chance for an R-wave to hit on just the right part of the T-wave and cause this rhythm. QTc > 500ms seems be associated with higher risk.
So what causes prolonged QT?
Many things can cause prolonged QT. The most common etiologies are electrolyte abnormalities and drugs. Hypokalemia, hypomagnesemia, and hypocalcemia are well known to cause prolonged QT. Potassium and calcium are included on the CMP but don’t forget about magnesium. Drugs are also a big cause of prolonged QT. The list of drugs is long. Probably too long to memorize. However, there are some common medications and medication classes that you should know. The big classes are, Antiarrhythmics (like Amiodarone), Antihistimines (like Diphenhydramine), Macrolides (like Erythromycin), Antipsychotics (like Haloperidol), and TCAs (like Amitriptyline). This is not a complete list, just some highlights. If you really want to know if a specific medication is associated with prolonged QT, www.crediblemeds.org is a good source.
Other causes worth mentioning are structural heart disease, cardiac ischemia, and stroke. Some people do have Congenital Long QT Syndrome, but this should not be the leading diagnosis in the ED. Also those people are still at high risk for developing Polymorphic VT.
How did our patient do?
Her medications were reviewed and she was not on any of the most common offenders. Then routine labs came back. Unremarkable, except for K of 2.9! Repeat EKG after potassium repletion.

EKG after K repletion
References:
- www.uptodate.com
- http://lifeinthefastlane.com/ecg-library/basics/qt_interval/
- http://hqmeded-ecg.blogspot.com/2013/10/polymorphic-ventricular-tachycardia.html
- bjsm.bmj.com/content/43/9/657/F3.large.jpgamp