![Room9er ["Room Niner"]:](https://room9er.com/wp-content/uploads/2020/03/cropped-Screen-Shot-2020-03-08-at-3.16.16-PM.png)
Small-bore Catheter (6-12 F) Thoracostomy Tube Placement
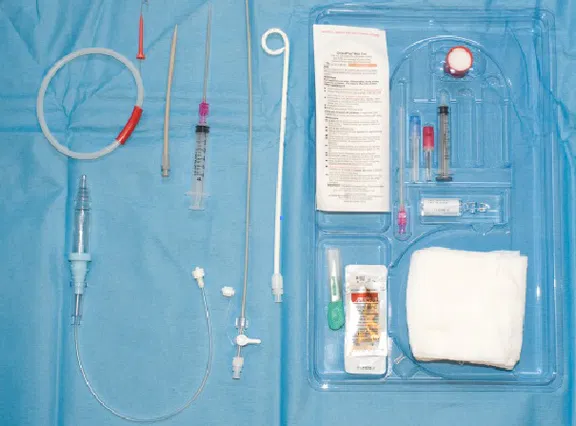
Small-bore catheter kit includes:
- Small-bore catheter (6-12 F)
- Trocar
- Finder needle with syringe
- Guide wire
- Heimlich flutter valve (one-directional)
- 11-blade scalpel
- Local anesthetic with additional needle and syringe
- Sterile drapes
- Sterilizing solution
Indications:
- Pneumothorax (especially stable, non-traumatic, spontaneous pneumothorax)
- Pleural effusion drainage in the unstable patient
- Large-bore chest tubes are still recommended for more viscous effusions such as empyema or hemothorax
Step-by-step Guide:
- Prepare the chest tube atrium and ensure appropriate length tubing is available for low wall suctioning once the procedure is complete
- Place the patient in either a lateral recumbent or supine body position with the head of the bed elevated to 30-45 degrees, or in a seated position with the patient leaning slightly forward for posterior tube placement (i.e. tube placement for drainage of pleural effusions, ultrasound guidance is recommended for posterior tube placement similar to with thoracentesis both to identify the location of the effusion and due to the increased presence of vascular structures between the rib spaces posteriorly)
- Identify the location of insertion, usually the 4-5th intercostal space at the mid-axillary line (similar to large-bore chest tube placement) at the level of the nipple. Remember the “safety triangle” bordered by the lateral edges of the pectoralis and latissimus dorsi muscles where there is a decreased risk for damage to underlying vascular, nervous, and organ structures
- Sterilize the skin surrounding the site of insertion and drape the patient accordingly using the drape provided in the kit, or by using sterile towels if preferred (remember to leave the nipple exposed to assist with identifying landmarks during catheter placement)
- Measure the small-bore catheter in front of the patient’s chest to determine the appropriate depth of insertion in a manner which ensures placement towards to superior aspect of the chest with all side ports within the pleural cavity (remember, the catheter can be withdrawn but not inserted further once the procedure is complete, similar to placing a central venous catheter)
- Generously anesthetize the skin at the desired site of insertion, advancing your needle deeper over the superior aspect of the rib to minimize the risk of damage to the neurovascular bundle, withdrawing prior to injecting lidocaine as the needle progresses through the soft tissue. Be sure to anesthetize the parietal pleural during this process, as it is fine for the needle tip to pass into the chest cavity
- Gently advance the finder needle over the superior aspect of the rib through the intercostal musculature similarly to the previous step while steadily drawing back against the syringe plunger as the needle tip advances. The plunger pressure will give way once access into the pleural cavity is achieved. Consider loading the finder needle syringe with several mL of sterile water for visualization of air bubbles in the syringe to assist with this step
- Once access to the pleural space has been achieved remove the syringe from the finder needle and insert the guide wire into the back of the finder needle passing the wire into the pleural cavity in such a manner that leaves most of the wire hanging outside of the patient
- Remove the needle from the patient and make a small incision in the skin at the base of the guide wire using the provided 11-blade scalpel
- Pass the dilator over the guidewire and into the pleural space feeling it give-way once it has pierced the parietal pleura and entered the thoracic cavity. Be sure to visualize the guide wire exiting the back of the dilator prior to insertion to ensure the wire is not accidentally lost within the chest. The dilator may be removed once this step is complete
- Pass the small-bore catheter within its trocar over the guide wire and into the pleural space in a manner that ensures all side ports are within the space. Generally, the first black indicator line can be used for small and thin patients, the second black line for the average adult, and the third black line for large adults. Similarly to the above step, ensure the guide wire is visualized exiting the back of the trocar prior to insertion.