![Room9er ["Room Niner"]:](https://room9er.com/wp-content/uploads/2020/03/cropped-Screen-Shot-2020-03-08-at-3.16.16-PM.png)
MICU Follow Up – Hypothermia
-ECMO (if available) may be best way to rewarm, 7-10 0C /hr
-Thoracic lavage up to 6 0C/hr
-If coding, can attempt defibrillation x 3; rewarm to at least 86 0 F
-Try to avoid stimulating heart, if need central access, fem line is best
-Rewarming complications include several electrolyte/coag abnormalities; check frequently
-Goal rewarm temp is 86-89 0F
Neuro Cases
- Stroke in Sickle Cell
-Neuro/hem consults early
-Exchange transfusion as treatment
-Can use upper motor neuron/lower motor neuron signs to help delineate where problem is
ex. UMN: +Babinski, spasticity, hyperreflexia ; LMK: Fasciculations, hypotonia, hypo/areflexia
2. Posterior Circulation Strokes
-Several symptoms: vertigo/dizziness, imbalance, unilateral limb weakness, dysarthria, diplopia, nystagmus, n/v, dysphagia
-HINTS exam can be used if symptomatic (Head Impulse, Nystagmus, Test of Skew)
-Subclavian Steal Syndrome: suspect in a patient with vertebrobasilar territory neuro sxs, arm claudication (exercise-induced arm pain or fatigue; coolness or paresthesias in extremity)
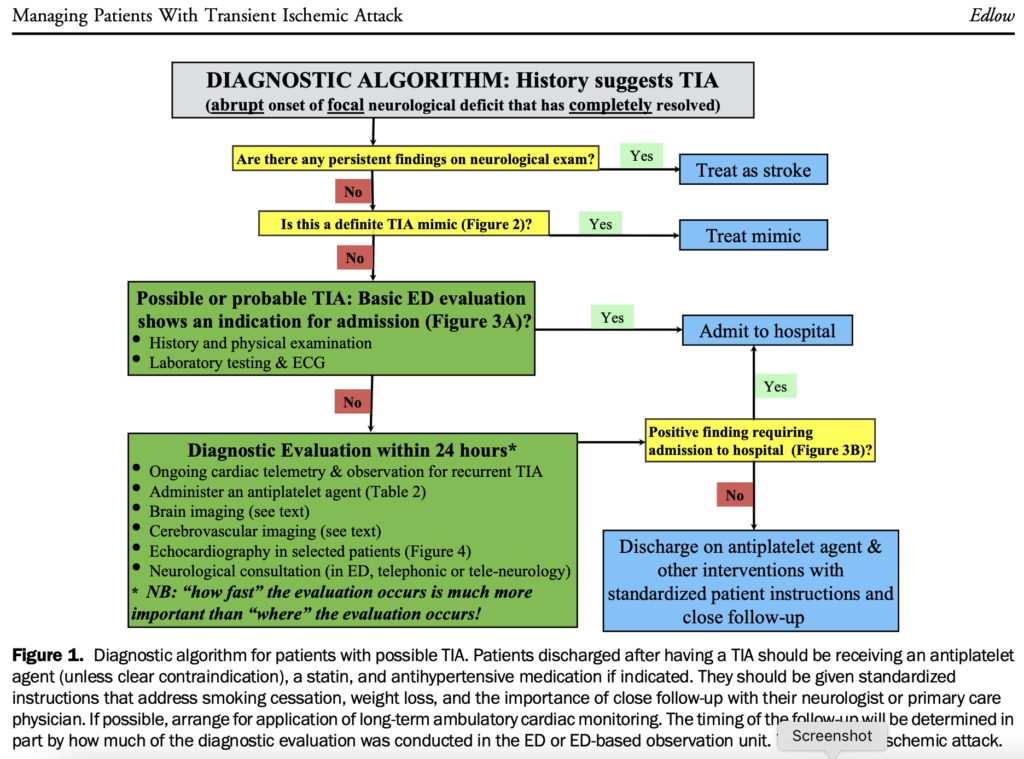
3) tPA
-BP goals for tPA administration <180/110 – may use Labetalol/Nicardipine for BP control
-Know some of the absolute contraindications; ex: any hx of intracranial hemorrhage, BP >180/110, known bleeding diathesis (platelet count <100,000; use of warfarin with INR > 1.7, use of DOACs) Can use MDCALC to run absolute/relative contraindications
-tPA symptom onset < 4.5 hours (prefer <3 hours esp in those >80 years)
Geriatrics Lecture
4 M’s for the ED: Medications
-Medications/polypharmacy should be high on differential for acute change in elderly
-1/3 of elderly patients lose independence in at least 1 activity when admitted
-Several meds are problematic; warfarin, ASA, plavix, digoxin, metformin and other diabetic medications, antibiotics
Room 9 Follow Up Case – Massive Hemoptysis
-Massive hemoptysis, no clear consensus definition. 100-1,000 mL/24 hours or >50 mL in a single event – really any bleed that is life threatening due to airway obstruction, hypotension, or blood loss
-Usually arises from bronchial circulation; MCC usually TB, bronchiectasis, lung abscess, bronchogenic carcinomas
-Airway protection: if having difficulty clearing airway or hypoxic/dyspneic, prepare for difficult intubation; intubation of mainstem of the good lung; can do this via going past the cords and turning ET 90 degrees; have patient lay on side of the bad lung
-TXA: nebulized TXA with 1 g TXA in 10 cc saline. Can also do 500 mg TID. Systemic route also an option, 1gm load in 100 mL NS over 10 minutes and 1 gm over 8 hours.
-Bronchoscopy and CT; CTA may help identify source; consults to consider early: Pulm, IR or CT surgery
EMS Lecture- PreHospital Stroke
-Several scoring systems (RACE, Stroke VAN, FAST-ED, CSTAT, LAMS) to help guide pre-arrival notification and transport to comprehensive stroke center
-CSTAT: Cincinnati Stroke Triage Assessment Tool, Screen for Large Occlusion Strokes >/= 2 is positive
Conjugate Gaze Deviation 2 points
Incorrectly Answers Age or Month and Does not follow at least one command (close your eyes, open and close your hand) 1 point
Arm (right, left or both) falls to the bed within 10 seconds 1 point
-Mobile stroke units – can decrease time to stroke tx by 50%, 20 units worldwide, CT scanner in back; tremendous expense without great improvement in outcomes
-tPA goal 60 minutes door to drug.