CORD/CDEM/EMRA/SAEM video on Transitions of Care. Take a look, consider using on your next rounds!
https://www.youtube.com/watch?v=7B7p_krIEkU&feature=youtu.be
![Room9er ["Room Niner"]:](https://room9er.com/wp-content/uploads/2020/03/cropped-Screen-Shot-2020-03-08-at-3.16.16-PM.png)
CORD/CDEM/EMRA/SAEM video on Transitions of Care. Take a look, consider using on your next rounds!
https://www.youtube.com/watch?v=7B7p_krIEkU&feature=youtu.be
An interesting case from the Pediatric ED:
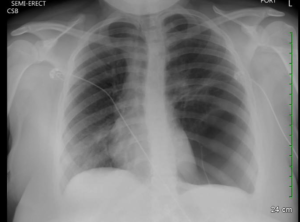
A mid teen female with a reported two year history of mild persistent asthma, presented with asthma exacerbation. She presented to an outside ED with two days of cough, wheezing and shortness of air which acutely worsened three hours prior to arrival. Upon initial presentation there, the patient was reported to be in moderate respiratory distress with increased work of breathing, tachypnea, and an O2 saturation in the 80%’s on room air. Lung auscultation revealed diminished breath sounds on the left with faint wheezing at left and right apices. She was placed on 3L nasal cannula with normalization of her O2 sats. She received an hour long course of albuterol and dose of Solu-Medrol, with moderate improvement in her symptoms. She subsequently received a chest X-ray which was concerning for a large left sided bleb/cyst with mediastinal shift to the right. Patient was subsequently transferred to us.
Further HPI and PMHx revealed that patient was diagnosed with allergic rhinitis in her early teens and diagnosed with asthma two years ago. She reported no history of ever being evaluated with a chest x-ray prior to current presentation. Over the course of the past two years she had been prescribed 3 courses of steroids and used albuterol approximately 2x per week PRN. Patient denied any other medical problems or smoking history.
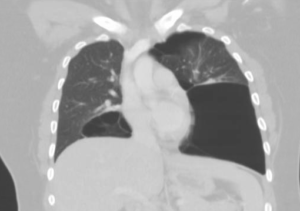
A CT scan of the chest confirmed presence of large left sided pulmonary cyst.
Patient was admitted and followed by both pediatric pulmonology and surgery. Inpatient workup included PFT’s and alpha-1-anti-trypsin (negative). She was eventually diagnosed with idiopathic giant bullous emphysema, otherwise known as vanishing lung syndrome. She later underwent bullectomy with improvement of her symptoms.
Bullous emphysema is often seen as a complication of COPD in adults, but rarely diagnosed in children with few case reports in the literature. Giant bullae can present asymptomatically, with progressive dyspnea, hypoxia or hemoptysis. Giant bullous emphysema is classified as occupying more than one third of a hemi-thorax, and is often initially mistaken as a pneumothorax on initial chest radiograph. As disease progresses, enlargement of the bullae fill with air and loss of lung function results as fibrous membranous surface of the bullae result in poor gas exchange. Bullae are at high risk for rupture and tension pneumothorax should be suspected if a patient develops worsening respiratory distress.
The learning point I took from this case is to step back and re-evaluate a patient’s presentation when things do not exactly add up, as in this case a teen with worsening asthma not responding to conventional treatment and little pcp workup in the past. This point is particularly exemplified in the pediatric population where we often see several low acuity cases each shift, often drifting into “auto pilot” mode, employing little critical thinking. Don’t forget, rare or more complex pathology may actually be responsible for the patients symptoms.
If I had to pick one case from intern year that truly taught me the importance of keeping a wide differential diagnosis, it would be my final Room 9 of the year. The buzzer went off, and as I made my way to the trauma bays, I was able to get a brief rundown from the attending. “Seizure, 40-sish male, no known history”. OK, this was something I could do. I began running everything I’d need to do through my head as I prepared for the patient. “ABC’s. Vitals. Fingerstick glucose. Ativan… Could be trauma, hypoglycemia, benzo or alcohol withdrawal…” As I was refining my differential, the patient came in. The patient was non-rhythmically jerking, was not responsive to voice or sternal rub. I noticed he was wearing dress pants and a collared shirt. He was breathing spontaneously and maintaining sats in the mid 90’s. Palpable pulses and good heart sounds. Glucose was in the 100’s. EMS said he had been found like this approximately fifteen minutes prior, and his clinical status hadn’t changed since then. No known medical history or medicines. I called out for the nurse to draw up Ativan, as I said this I noticed the patient had urinated on himself. Everything in my mind pointed towards a seizure. I grabbed the otoscope to perform the secondary survey and pried open his eyes. That’s when I felt the rug come out from under me.
The patient had pinpoint pupils, one millimeter bilaterally. The attending and I immediately had the same thought, and as I opened my mouth I heard him say, “let’s get some narcan for this guy!” The narcan got administered quickly, and soon after the patient woke up agitated, but responsive. His family had driven to the ED soon after he arrived, so questioning him was difficult. We ended up taking him to privacy in an empty x-ray room, where he admitted to using heroin earlier in the day. Sure enough, his toxicology screen was positive for opiates. We counseled him, observed him in the ED to ensure he didn’t need another dose, and then discharged him home.
What struck me about this case was that while I had formulated a differential, I had done so after anchoring to a faulty premise. It taught me a valuable lesson in keeping my differential broad, and it’s a lesson I’ll carry to every patient encounter from here on out.
I had a fairly interesting patient back in November 2016 when I was at Jewish. I had picked up a patient with chief complaint of chest pain after an attending handed me the EKG below. The patient was being rolled back from triage to a room at the attending’s request. 42yo AAM with history of hypertension, hyperlipidemia, diabetes, sleep apnea and CAD status post CABG in 2008. The patient was complaining of chest pain that initially started when he was sitting at home watching TV about an hour prior to arrival. He described the pain as sub-sternal and radiating to his left arm. He had associated SOA, palpitations, and diaphoresis along with the pain. He was also nauseated since the onset of pain.
Pretty classic presentation here in a patient with previous heart disease. His initial EKG recorded in triage is below:
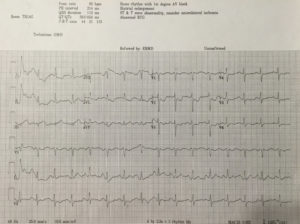
Upon review, you can appreciate that there may be ST elevation in III. Also, ST depressions are noted in the precordial leads along with ST changes elsewhere. My question to all of you based upon reviewing this EKG: Would you call this is a STEMI and would you activate the cath lab at this time?
The attending that I was working with at the time didn’t feel that we could definitively call this a STEMI based upon the first EKG. We examined the patient and collected his history after he was brought back. After labs were collected, the patient received nitro paste. Despite the paste, he continued to have pain. After approximately 15 minutes of being in the back, the patient reported that his pain was worsening. The decision at that time was made to get a repeat EKG. The repeat EKG is below:

So now what are your thoughts? There is obvious ST elevation in the inferior leads. There are also ST depressions in the precordial leads. This EKG was taken 34 minutes after the first EKG which was performed in triage. Through these two EKGs, you can appreciate the evolution of a STEMI. This patient was emergently taken to the cath lab at that time and underwent left heart cath. He underwent an impella-assisted PCI to his SVG-PDA and was started on dual anti-platelet inhibitors. Following his PCI, he also had an episode of wide-complex rhythm which resolved after receiving amiodarone.
So this patient who was found to have a STEMI on his repeat EKG had presented with an initial EKG that was non-diagnostic for his condition. Did this affect his outcome in any measure? What can we learn from this?
According to a 2013 study conducted by Riley et. al, in a national sample of patients diagnosed as having STEMI (41,560 patients), 11.0% had an initial non-diagnostic ECG. Of those patients, 72.4% had a follow-up diagnostic ECG within 90 minutes of their initial ECG. There did not appear to be clinically meaningful differences in guidelines-based treatment or major inhospital outcomes between patients diagnosed as having STEMI on an initial ECG and those diagnosed on a follow-up ECG.
So, did the additional 30 minute delay in activating the cath lab affect this patient? Likely not. However, what this case reinforces is the importance of a repeat EKG as 11% of these patients likely will not have STEMI on their first EKG.
References:
Am Heart J. 2013 Jan;165(1):50-6. doi: 10.1016/j.ahj.2012.10.027. Epub 2012 Nov 21. Diagnostic time course, treatment, and in-hospital outcomes for patients with ST-segment elevation myocardial infarction presenting with nondiagnostic initial electrocardiogram: a report from the American Heart Association Mission: Lifeline program. Riley RF1, Newby LK, Don CW, Roe MT, Holmes DN, Gandhi SK, Kutcher MA, Herrington DM.
Recent EMRAP podcast reminded me of a case from when I was a Medical Officer in the Navy.
One of my Marines, early twenties, with no medical problems presented for follow up in sick call after being seen in the emergency department for a headache. Since it was the worst headache of his life, an LP was performed. Both the LP and the CT head were negative. He was given standard headache treatment with “migraine cocktail” from what I remember, however, no significant relief.
He presented to clinic with complaint of ongoing headache that was only better if he laid completely flat with excruciating pain with sitting up. He refused to do anything other than lay on the gurney in the treatment room.
His presentation was classic for post LP headache, however, he states that this was the same headache that he presented to the ED for the previous evening and was not changed by the LP. He was adamant about this timeline and unchanging symptoms after LP. Physical exam was normal to include normal Neuro exam.
I subsequently called the Neurologist on call at Naval Hospital, who stated the likely diagnosis was a “spontaneous CSF leak” and recommended a blood patch. I was quite confused as I had never heard of such and it seemed like a made up diagnosis to me at the time. I did, however, want to help my patient and for him to leave the clinic at some point that day. I then called anesthesia who was agreeable to the blood patch given recent LP and current exam/symptoms. The patch lead to resolution of his symptoms and he was able to stand up and walk without a headache.
This is the only case that I have seen, however, the recent EMRAP review leads me to believe that I might see another case while practicing Emergency Medicine.
SIH is caused by a spontaneous tear in the dura in the spine or elsewhere in the meninges and leads to intracranial hypotension from CSF leak. Symptoms are incredibly similar to post LP headache given the pathophysiology on really differ in that CSF leak in an LP is iatrogenic and SIH is well, spontaneous. Diagnosis can be by LP, which will demonstrate low opening pressure, or MRI of the Brain W/WO and Spine W/O which will demonstrate the leak. The symptoms are similar regardless of the level at which the leak occurs so you may have scan the entire meninges to find it.
Treatment initially is caffeine and rest for mild-moderate headaches and lumbar blood patch for moderate-severe headaches.
Uptodate has a lengthy but throughouh algorithm for diagnosis and treatment. If lumbar patch doesn’t work, a more targeted approach may need to be employed.
I’m currently on peds anesthesia and behind on reading Annals, which worked out in my favor. I was looking through the February 2017 issue and there’s an EM:RAP commentary about the neonatal airway. So I figured I would give you all the highlights from that article.
…forever seeking the unsuspecting emergency medicine intern.
A previously healthy teenage male presented to the emergency department via emergency medical services with the complaint of weakness, sensory changes, and increasing difficulty of breathing. Family reported the patient went outside to mow the grass approximately 10 hours prior to presentation. After two passes in the yard with a push mower, the patient had sudden onset occipital headache, fatigue, parasthesias described as tingling in both lower extremities, and generalized weakness. Patient reported these symptoms to parents and laid down to rest. After an hour long nap, patient was encouraged to take a shower to see if symptoms improved. During shower, patient became weaker, had one episode of vomiting and was no longer able to stand on legs. The patient’s father reports patient was able to make small movements but unable to ambulate or push against resistance. Emergency medical services were contacted at this point, however, after assessment, the symptoms were deemed related to anxiety and patient was not transported. Over the course of the day, the patient’s weakness progressed to the complete inability to move legs, followed by inability to move arms, with continued paresthesias in all extremities. After patient demonstrated worsening respiratory distress, EMS was called again. Parents denied history of asthma, prior wheeze, fevers, recent illness or trauma, recent travel or drug abuse. Family reports patient went camping one week prior but denies tick exposure.
On exam, the patient had significant respiratory distress with poor air movement and was only able to answer questions with one word responses secondary to respiratory distress. Neurological exam revealed 0/5 strength in all extremities, areflexic biceps and brachioradialis reflexes, areflexic patellar and Achilles reflexes, and downward going Babinski bilaterally. Sensation to light touch was intact but diminished in all extremities. There were no rashes or lesions on skin exam.
Initial differential included but was not limited to:
As concern for bronchospasm, the patient was given IM epinephrine and started on a hour long albuterol while history was being obtained. Bedside ultrasound demonstrated grossly normal myocardial contractility without effusion, normal lung sliding, and a collapsible IVC. Chest x-ray was unrevealing. After lack of improvement with initial intervention, second dose of epinephrine and fluid bolus begun. Intial VBG demonstrated hypercapnea and patient was started on BiPAP. Within minutes, patient showed improvement in respiratory status and appeared more comfortable. Initial CMP, CBC, CRP, and ESR were unrevealing. Lumbar puncture was performed after head CT revealed only an arachnoid cyst. CSF studies demonstrated mildly elevated segs, mildly elevated glucose, negative gram stain and normal protein. Foley catheter was placed after patient complained of bladder fullness (confirmed by bladder scan) with inability to void. Neurology and Neurosurgery were consulted from the emergency department, who requested urgent MRI on admission. Patient was admitted to PICU with ED diagnoses of acute flaccid paralysis and acute neuromuscular respiratory failure. After admission, MRI was obtained and demonstrated (drum roll please) ischemia vs. infarct from approximately C2-T5 with predominance in the anterior horns.
The literature review of non-traumatic spinal cord infarction is as rare as the pathology itself in the pediatric population and predominately consists of case studies. Causes typically include but are not limited to hypotension, vascular injury, thrombus, embolus or compression. Considering many of these etiologies are already scarce in the pediatric population, finding cause proves to be a difficult task. Pain in neck, back or legs, weakness, tingling, and numbness are commonly described symptoms in pediatric case studies and were present in the patient that presented to us. Prognosis studies have been performed on primarily adult patients; one such study demonstrated >40% recovery in ambulation amongst the 37 patients that left the hospital wheelchair bound through aggressive physical therapy and rehabilitation programs.[1] Poor prognostic factors include female sex, advanced age, severity of symptoms, and lack of improvement within 24 hours after infarction.[2] It appears as though outcomes are primarily dependent on access to physical therapy and supportive care including psychological treatment. Workup and treatment recommendations if suspicious of atraumatic spinal cord infarct include obtaining an MRI for definitive diagnosis, followed by autoimmune, hypercoagulable, and infectious evaluations. Treatment in the emergency department is mostly supportive and includes addressing any contributory conditions and the management of respiratory concerns.[3]
On follow up, I found that the patient required intubation after exhibiting respiratory decompensation after the MRI was obtained. Initial treatment with high-dose steroids and IVIG were discontinued when infectious and immunologic work-ups were unrevealing. The hospital course was complicated by neurogenic bowel and bladder, neuropathic pain, anxiety, intermittent autonomic instability with hypotension, pneumonia and a urinary tract infection. The patient required tracheostomy and percutaneous gastric tube placement during his hospital stay. The patient continued to exhibit flaccid paralysis of all four extremities and ventilator dependence on discharge to acute rehabilitation.
Per my own investigation, I was relieved to find that Frazier has both success managing these cases and many unique resources that may positively impact this patient’s course (if you are curious here is some video evidence https://www.youtube.com/watch?v=8o_w174rI3s). Needless to say, my differential for motor weakness, particularly in pediatrics, will forever be haunted by this case.
[1] Robertson CE, Brown RD Jr, Wijdicks EF, et al. Recovery after spinal cord infarcts: long-term outcome in 115 patients. Neurology. 2012; 78: 114–121.
[2]Cheshire WP, Santos CC, Massey EW, Howard JF Jr . Spinal cord infarction: etiology and outcome. Neurology. 1996;47(2):321.
[3] Spencer, Sandra P. MD; Brock, Timothy D. MD; Matthews, Rebecca R. MD; Stevens, Wendy K. MD. Three Unique Presentations of Atraumatic Spinal Cord Infarction in the Pediatric Emergency Department Pediatric Emergency Care. 30(5):354-357, May 2014.
Last month I had an interesting Room9 for visual purposes. The story per EMS was jumbled, as it can be from time to time. All we knew was that the patient was a middle aged man who either fell off a roof or jumped off a ladder into a foot and half of water. …agreed. Details were otherwise unavailable. We manage repercussions of injuries, not the causes.
The patent came in intubated, wet, hemodynamically stable. The patient had ketamine en route but was still active with GCS 6T. He required more than your typical sedation to be amenable for the CT scanner. The physical exam showed no motor activity in lower extremities, including to painful stimuli. We noted no step-offs or abrasions. The patient had no signs of trauma other than the motor weakness.He moved his upper extremities and needed restraints due to lack of response to sedation. CT images are below. Most of these images mirror almost exact images from Dr. Ferguson’s lecture on spine fractures, thus I thought it would be good to go over.

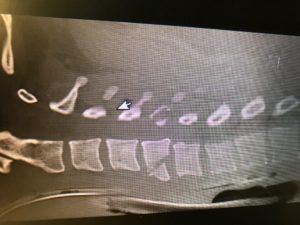

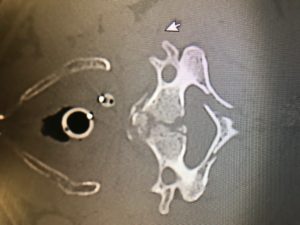
As you can see the patient had significant fractures of his cervical spine. Talking with Neurosurgery, the burst fracture is more common in lower thoracic and upper lumbar spine and only is seen in cervical spines to this degree under severe axial load injuries, such as going head first from a significant height (especially when the posterior column has a vertical fracture as seen above).
I’ve always wondered the significance of doing spinal check during the physical exam prior to CT, when they are already getting “manned”. I often feel that if there is real pathology (ie. unstable fractures), won’t palpating (and deep palpation on obese patients) worsen the fracture and theoretically cause neurological issues. I haven’t found much to substantiate that, but it seems to make intuitive sense; I am open to any other opinions / suggestions.
Does anyone want to comment on the type of fractures noted, stable vs unstable (refer to Ferguson’s lecture)?
Are teardrop fractures stable?
Is there any significant retropulsion?
Could you hypothesize flexion vs extension injury?
Answer: Unstable teardrop fracture as well as a burst fracture, and borderline chance fracture (not typical for this cervical spine location).
For further spine related information please look at the links below or Dr. Ferguson’s spine lecture. Ferguson’s is a great source covering the importance of stable and unstable fractures, and a great lecture for interns to go over, especially early on in the year.
Here is a good podcast from Scott W. on less traumatic c-spine injuries:
EMCrit 63 – A Pain in the Neck – C-Spine Imaging and Clearance
And some other good sources:
http://www.aafp.org/afp/1999/0115/p331.html
http://www.paems.org/pdfs/online-ce/Evaluation-and-management-of-acute-cervical-spine-trauma.pdf
All,
As we have started to move towards shorter, more concise lectures I thought I would share these brief talks from EMRA. I encourage you to at least watch the first lecture (if not all three).
I want to point out how the first speaker uses essentially no bullet points, slides with minimal words, and images that cue him into what he’s talking about, cue the audience as well, but aren’t insanely distracting so that his audience is listening to him and not reading his slides. He also does a great job at the end of summarizing his talk (again with no bullet points).
I’d like you all to consider this when creating a talk, however big or small and if you have questions/need anything regarding talks fell free to ask me. I may try posting more tips/pages like this in the future if you find it helpful.
We have noticed more and more this culture in our ED of obtaining an initial ECG, an initial troponin, and then waiting 2 or 3 or 6 hours to obtain a second troponin only and then discharge if negative.
I dove into the literature and wrote this post to address the SECOND ECG AT TIME OF SECOND TROPONIN as part of a rule out strategy for low risk ED patients.
I will not even address the fact that people are not obtaining a 2nd ECG at time 20-30 minutes from the first. This is on UpToDate, in ACC guidelines, in ACEP guidelines. It is simply standard of care to obtain an early, repeat ECG on anyone you remotely suspect of having ACS. I harp on this in lectures and have posted on it before. I also will not be talking about hs-Troponin (high sensitivity troponin). Many articles and FOAMed commentaries have covered hs-Trop, and we do not have this test at UL. So please do not think you can rule out all comers with 1 troponin, because you need the hs-trop to even consider this.
This post relates to the issue of a repeat ECG at time 2hr or 3hr (I am not a 6 hour guy, I like the 2 or 3 hr depending on symptom time frame). Don and I discussed the 2nd ECG phenomenon and he said it is just our culture at UofL, hence inspring our Room9ER post. Well we need to change the culture.
Now I didn’t want Geralds to cherry-pick an article to try to rebut me on this, so I went down a rabbit hole of ACS rule out, nSTEMI, HEARTS, TIMI and cardiac markers.
If your attention span is reaching its limit here is the bottom line:
All rapid rule out tools and their validation studies involve at least a SECOND ECG with the repeat troponin. HEARTS, ACC/AHS guidelines, TIMI-based rule outs, etc.
I was early to drop the CK and CK-MB on initial and repeat marker testing in favor of solely the troponin, but dropping the ECG is irresponsible. And is not evidence-based.
Below are many quotes and a figure, then a letter to the editor, from various sources. It was actually somewhat difficult to find in the methods exactly when or even if a repeat ECG was done. Much of the time, the ECG done at time of 2nd trop was not even the 2nd ECG, as mentioned above. “Serial ECGs” is the rule. It seemed as though the repeat ECG(s) were implied in the study, and that the research question was simply timing a troponin.
Dr Huecker composed most of this post because Dr Bertolotti is so excited about and diligently preparing for Research Day.
Enjoy, and please post comments!
— Patients with probable or possible ACS but whose initial 12-lead ECG and cardiac biomarker levels are normal should be observed in a facility with cardiac monitoring (e.g., chest pain unit or hospital telemetry ward), and repeat ECG (or continuous 12-lead ECG monitoring) and repeat cardiac biomarker measurement(s) should be obtained at predetermined, specified time intervals (see Section 2.2.8). (Level of Evidence: B)
— The c-statistic of troponin only was 0.70. With addition of the ECG the c-statistic improved significantly to a value 0.78, with a likelihood ration test p-value of <0.001
— Anderson et al. JACC Vol. 50, No. 7, 2007 ACC/AHA UA/NSTEMI Guideline Revision August 14, 2007:e1–157 If the initial ECG is not diagnostic but the patient remains symptomatic and there is high clinical suspicion for ACS, serial ECGs, initially at 15- to 30-min intervals, should be performed to detect the potential for development of ST-segment elevation or depression. (Level of Evidence: B)
— ACEP (What will be used for or against you in court, as the case may be)
Acute Coronary Syndromes (Non–ST-Segment Elevation – Adult)
Critical Issues in the Evaluation and Management of Adult Patients with Non–ST-Segment Elevation Acute Coronary Syndromes (September 2006)
Complete Clinical Policy on Non–ST-Segment Elevation Acute Coronary Syndromes (PDF)
Scope of Application. This guideline is intended for physicians working in hospital-based emergency departments (EDs) or chest pain evaluation units.
Inclusion Criteria. This guideline is intended for adult patients presenting to the ED with suspected non–ST-segment elevation acute coronary syndromes.
Exclusion Criteria. This guideline is not intended for pediatric patients, patients in cardiogenic shock, or patients with injury on the initial 12-lead electrocardiogram (ECG).
Critical Questions
— Letter: Re: “Troponin-negative chest pain”—a diagnostic evasion?
This brief article is well written and I agree the diagnostic label of ‘troponin negative chest pain’ is unhelpful. However the article repeats some common misconceptions which require correction.
Firstly, the article implies that the majority of patients attending hospital with chest pain have an acute coronary syndrome. This is absolutely not the case – in fact most patients with suspected acute coronary syndrome do not have it. (1) Often patients receive a label of acute coronary syndrome and this is later corrected by the cardiology registrar or consultant on call – although by then it may be too late to change the patient’s perception that they have ‘had a heart attack’.
Secondly, there appears to be a misunderstanding of the value of troponin testing. Troponin assays are positive when there has been myocardial necrosis. They do not give any information about the mechanism of myocardial necrosis – a positive troponin can indicate acute coronary syndrome, but may also occur in heart failure, prolonged arrhythmia, sepsis, pulmonary embolism and many other situations. (2)
Similarly, a negative troponin does not absolutely exclude a cardiac cause for symptoms – nor does it mean the patient is necessarily in a low risk group. (3) Patients with unstable angina, dynamic ECG changes, but negative troponin should be considered as having a similar risk of mortality and morbidity to those with a normal ECG but a positive troponin.
Troponin assays should generally be considered a prognostic, not a diagnostic test, and should be used in conjunction with the patients history and ECG – never alone.
Every resident must listen to this podcast (or watch this video) at once. I finally listened to it and was pleased to find it a concise, evidence-based and accurate talk. I avoided watching because I thought he would talk about how much he loves his droperidol and that we should all use it, which would fill me with unbearable envy, since we have not had it in Louisville for years. I have been aware that no US company manufactures it but many EM / FOAMed docs still talk about it. Well Dr Strayer now has no access to the drug and shares his disappointment.
Take home points:
No but seriously many great points related to managing the combative patient. From the mildly disorganized schizophrenic, all the way to the truly medico legally dangerous excited delirium, Strayer gives inarguable advice. I love the “shove an O2 mask on the patient who is being restrained by 6 security guards.” He notes that this will often calm the patient, it will protect from spitting, and it will oxygenate the patient. Many other practical pearls here that you WILL USE pretty much every shift at UofL.
Post your favorite tips in the comments.
Hey All,
Saw this recent post on REBEL EM and wanted to post it as a follow up to Dr. Bosse’s lecture this past week on Salicylates. Will take ya 5 minutes or less.
Acute Salicylate Toxicity, Mechanical Ventilation, and Hemodialysis