![Room9er ["Room Niner"]:](https://room9er.com/wp-content/uploads/2020/03/cropped-Screen-Shot-2020-03-08-at-3.16.16-PM.png)
Here is the Micronutrient Wellness lecture.
Monthly Archives: December 2016
How Evidence Based Are We?
Here is a pretty comical article by Dr Ioannidis. If you do not know who this is stop now and read this.
This article was just published. It is written as a report to the father of evidence based medicine, Dr David Sackett. It takes a not terribly optimistic view of the current state of medical research. He calls out industry bias, ghost authorship, and many other flaws of our system. We are very lucky to have people like Dr Ioannidis ensuring integrity to the research process.
QTc
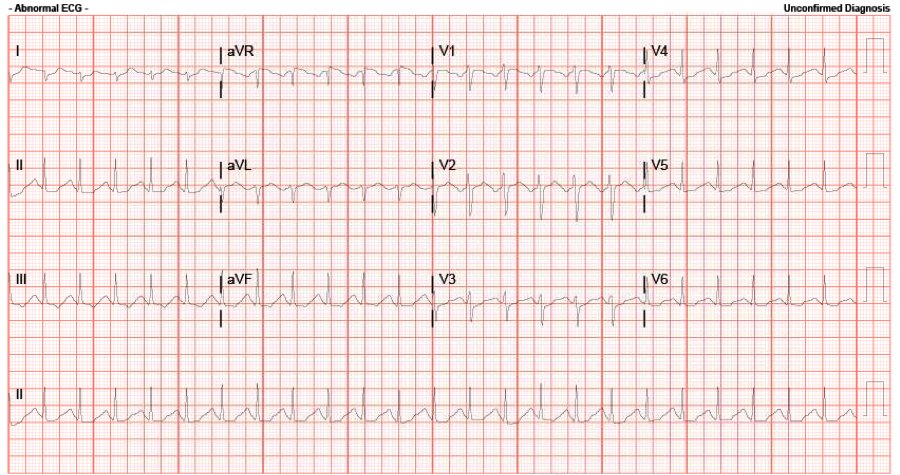
Yesterday I had a 21 yo female come in by BLS crew, tachycardic with a GCS of 3, spontaneously breathing with equal and reactive pupils bilaterally at ~ 6mm, with vomitus around her airway. She was found down at home after her significant other called EMS due to concern that she was going to attempt suicide. Report received that she was found with multiple empty pill bottles nearby. No response to Narcan either in the field or in Room 9.
Here is her ECG: Calculated QTc (automated) is 401 ms, rate is 143. The accepted normal value for QTc is: below 450ms for men and below 460ms for women. The 99th percentile of normal: 470ms (men) and 480 ms (women).
Just how does the computer calculate this?
By using the Bazett formula: QTc = QT / sqrt( R-R interval in seconds)
This means of course that if our rate is 60 BPM, then our R-R interval would be 1000ms, (or 1 second), and thus our QTc = QT/sqrt(1); and therefore in this situation QTc equals QT.
In our particular case: the R to R interval is 10.5 boxes (thus 420 ms, or in seconds: 0.420). The QT was autocalculated at 260 ms, and when using the Bazett equation, this gives us a QTc of 401 ms.
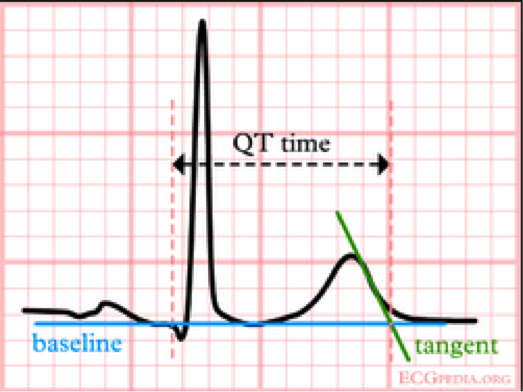
What if you cannot rely on the computer calculated QT (which certainly can be inaccurate)? Then calculate the QT yourself by finding the tangential intersection of the T wave downslope with the ECG baseline, and measuring the intersection distance from the start of the QRS. See the diagram below:
Using this measurement principal, and (in our case) using the lead V2 where the p wave and T wave are 180 degrees out of phase, we obtain a QT ranging from 8-9 boxes (320-360 ms). When using the Bazett, this gives us a calculated QTc of 493-555. Of course qualitatively we can tell the QTc seems long as it exceeds half the R-R interval, quantitatively this is an increased QTc of 38% from the auto calculated, and is certainly in the significantly prolonged QTc range.
Follow-up: TCAs and benzos positive on her drug screen. She was started on a bicarb drip in the ED (placed 3 amps of bicarb in a bag of D5); pH 7.34, lactic acid 1.2. She is supposedly on Flexeril (similar in structure to TCA and will light up as TCAs on the drug screen), treated the same, however appears to be less cardiogenic in toxicity:J Emerg Med 1995;13(6):781-5. Pt is intubated and stable currently.
Click here for the EMCrit on TCAs (overview below):
- Bicarb drip: Goals: QRS duration <100, hemodynamically stable, Na ~150, pH ~7.5. Sodium and bicarb don’t rise significantly in severe toxicity, her repeat showed no change in either.
- Magnesium: may help, though risk of Torsades is low as long as the patient remains tachycardic.
- Lidocaine: even though lidocaine is another Na-Channel Blocker, it will antagonize the effects of the TCA-like medications.
- Watch the electrolytes (decreases expected in both K+ and Ca+): Lytes and ABG Q1H; (My pt’s Ca+ dropped from 9.8->8.5 over 4 hours).
- Intubation: hyperventilate to ensure no hypercapnia (want alkalosis). Sedate with versed or propofol to raise seizure threshold.
- ECMO: If everything else fails.
Good read on HEART Score
Can you give Vasopressors through a PIV?
I looked back and couldn’t find a post about this topic in the last year or so but forgive me if it has already been posted. I have been following R.E.B.E.L. EM for a few months now and I would recommend it to everyone who has the time and wants quick summaries on the latest EM literature. They have short written summaries of papers including pros/cons of the study and what they feel are the most important take away points. It was founded by Salim Rezaie with Rob Rogers, Matt Astin and Anand Swaminatham serving as editors.
Occasionally they will have a “mythbuster” post looking at common myths in the ED and the most uptodate literature available on the topic. (their latest mythbust is on “safe” glucose levels before ED discharge but I digress)
Back in May they reviewed the safety of vasopressors through a PIV. The topic paper was titled “A systematic review of extravasation and local tissue injury from administration of vasopressors through peripheral intravenous catheters and central venous catheters”
What the review found was very interesting: of 318 events, 204 results in local tissue damage, 114 were only extravasation events and 7 events involved the use of a CVC (so clearly not completely safe). Interesting, of the 204 local tissue events 85.3% involved PIV distal to the antecubital fossa and 96.8% involved administration of >4hrs.
REBEL EM’s take away points were:
In critically ill patients, with hemodynamic instability, vasopressor infusion through a proximal PIV (antecubital fossa or external jugular vein), for <4hours of duration is unlikely to result in tissue injury and will reduce the time it takes to achieve hemodynamic stability.
What I feel like this means for us is simple: If you have a crashing, hypotensive patient who needs a pressor without a CVC but good proximal PIVs, start the pressor immediately, stabilize the patient as best you can, then take the time to properly place a CVC.
Continue to monitor the PIV until it can be switch to the CVC and stop the pressor immediately if there is any suspicion for local extravasation. I am sure this will make some people nervous but I think this is better then placing a “crash line” that is less then sterile which will expose an already ill patient to infection or other complications secondary to a hastily placed CVC.
I highly recommend read their review and how they came to this conclusion along with their other posts. I have included the link to this study at the bottom.
http://rebelem.com/mythbuster-administration-of-vasopressors-through-peripheral-intravenous-access/
Name that Disease?
55 y/o F with hx of HTN,COPD and recurrent indurative lesion on her left foot, last event was a yr or so ago, presented to the ED for worsening pain and increased size of her lesion for the last few wks now. No fever, chills, or fatigue. On exam, the cutaneous lesion is mildly tender and erythematous, non-fluctuant, no warmth noted. Pt is immunocompetent.

/
/
/
/
/
/
/
/
/
/
/
/
Answer:
Pyoderma Gangrenosum. Take home point is to not I&D this lesion. It is not an abscess. It is a rare autoimmune disease that affects pts in their 40s-50s. These pts will have hx of other autoimmune diseases–lupus, crohns etc. An I&D would lead to phenomenon known as pathergy, the formation of new lesions following a trauma.
Tx: High dose steroids and pain meds. Refer to podiatry. Pt in this case was already well known to podiatry on arrival and was discharged with steroids and pain meds after podiatry consult in the ED.