![Room9er ["Room Niner"]:](https://room9er.com/wp-content/uploads/2020/03/cropped-Screen-Shot-2020-03-08-at-3.16.16-PM.png)
20 yo M with unknown PMH comes in to room 9 with AMS and tachycardia to the 180s. Per EMS, he had been found down in his apartment, with crack cocaine pipes and other drug paraphernalia around him. He was found to be tachy as mentioned, as well as febrile with a temp of 103 axillary.
When he arrived in room 9, his HR was still in the 170s-180s. Blood pressure normal. He was pale, diaphoretic, and looked sick. He was speaking inappropriate words and would localize pain, GCS 12. Pupils dilated and briskly reactive. Rectal temp 104.1. CXR normal. Started IVF bolus and placed ice packs to the groin and axillae. Also gave Ativan as this was likely a stimulant overdose.
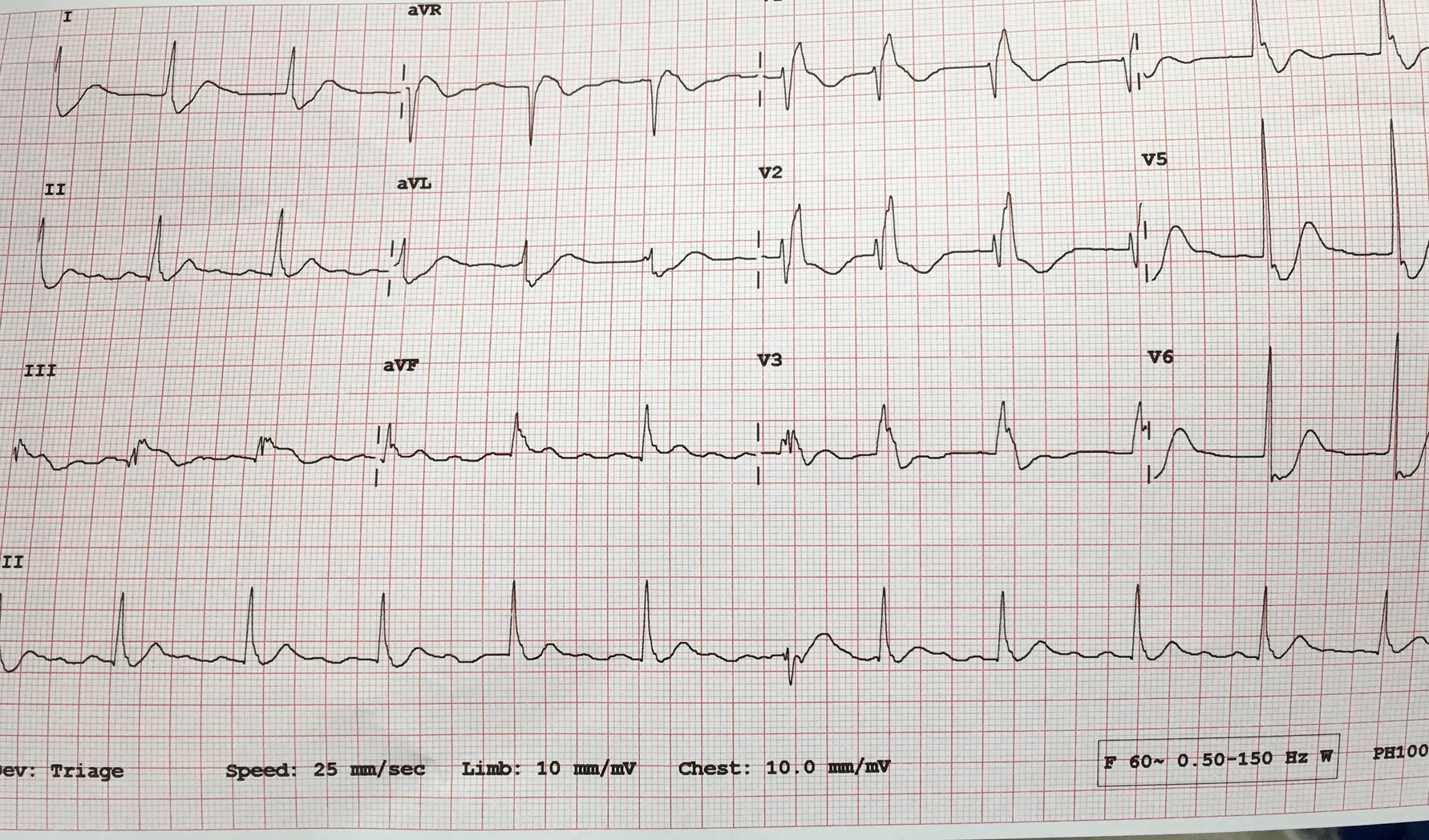
First EKG showed SVT at 180 BPM. After 2L of crystalloid and ativan, a repeat EKG showed sinus tachy at 140. The pt’s mental status was unchanged. The iStat showed a lactate of 13.
The plan was to place a rectal probe and monitor his temp, give him more fluids and Ativan prn, and re-assess later. I thought this was 100% an overdose. No problem.
About 2 hours and who knows how many room 9s later, I go to review his labs. I haven’t heard anything from nursing other than him continuously pulling out his rectal thermometer probe, so all must be well…Turns out he has a WBC of 44,000. Lactate has trended down, but he is still febrile to 102. This is when it hits me that maybe the guy who I’ve been treating for stimulant overdose is actually septic? His CXR and UA were normal, but maybe he has meningitis or encephalitis and that’s the reason for his mental status? Maybe I’m now 2 hours late with ABx?
I suppress the awful feeling in my stomach and go re-evaluate the pt. His mental status is unchanged from when I saw him in room 9. At least now his HR is in the low 100s. Given his mental status and tenuous vital signs, I know this patient is going to have to come in to the MICU. He’s going to need a head CT and an LP to rule out meningitis. I gave him antibiotics and called MICU. They evaluated the patient, and they agreed.
I chart checked the patient the next day. His LP was normal. His mental status improved overnight and he was transferred to the floor. Turns out this actually was likely all tox-related, but I thought it was a good learning point nonetheless. Sometimes it’s convenient to go down the path you’re led to by EMS or by nursing. Not only is it easy, but it’s usually the right path anyway. The stroke buzzer goes off and you immediately get your quick assessment over with so the patient can go to CT and stroke can do their thing. EMS tells you they found the patient in a house with drug paraphernalia, so you run with that.
But it’s important to keep the differential wide open when you first see a patient. At least consider less likely and less obvious possibilities. At some point, you’ll catch something that you otherwise would have missed until it was too late.