So I’ve had to encounter my two sickest patients in the holding area within the past 2 weeks or so. One was a reminder from intern year while looking through spice charts, while the other was an actual patient that I had 3 days ago.
We always tend to take the “Tank” patients lightly and overlook them sometimes. I just want to use this as a warning (especially to the interns) that sick patients can also use heroin/ETOH/Spice, so pick up on the small interactions that don’t go right. I’ll try to present these starting with how their chief complaint lead to the final diagnosis.
Patient 1 (intern year)
- middle aged male
- CC: Spice OD, Nausea/Vomiting
- Final Diagnosis: Subarachnoid Hemorrhage
- Time to Diagnosis: 7 hours
So this guy presented as a spice reaction. This was before spice became as widely spread as it is now, and no one knew what to expect symptomatically (not that there is ANYTHING that is characteristic to spice anyways).
General story from talking with this guy is that he used spice for the first time that night. No significant past medical history. He was on a first date where everything had been going well. He had borrowed some spice from his friend where he used back at his place after dinner. Soon after he started having nausea and projectile vomiting and was acting ‘goofy.’ At that his date called EMS and the date ended.
Exam:
- Gen: Fully A&O, slightly odd in that he seems incredibly happy to be here
- CV: RRR
- Pulm: CTAB
- ABD: NT/ND
- Neuro: CN II-XII intact, motor intact, sensation intact, ambulates without difficulty to bathroom
This man was like most of our intoxicated patients–a sober re-evaluation. At approximately 2 hours he was still vomiting in the ED, so the medical workup was initiated. Due to his odd behavior with vomiting, we got a CMP/CBC/Tox & CT Head. The night continued busy and I almost forgot about him as I waited for results. Ultimately he never got his CT Head due to being uncooperative but I wasn’t told until hours later. He ended up getting Geodon/Ativan in the ED but instead of calming him down he became more agitated and was no longer oriented. Ultimately getting rolled into room9 to be intubated prior to CT and the final diagnosis was made.
Certain forms of spice that lead to agitation also lead to spikes in blood pressure, and there are a few case reports of significant hypertension occurring after spice use. This guy had the unfortunate case of rupturing an aneurysm after using spice likely from a BP spike. I’m honestly not sure if the outcome would have been any different had I reached the diagnosis sooner — he got repetitive Head CTs and ultimately an EVD on hospital day 3. I didn’t really take him seriously even after I ordered a lab workup. This really changed my perspective on patients being held for intoxication. He spent 1.5 months in the hospital (1 month intubated) before being discharged to rehab.
Patient 2
- Middle aged white female
- CC: Heroin OD got Narcan
- Final Diagnosis: Cardiogenic Shock
- Time to Diagnosis: 3.5 hours
This case I handled a bit better (I’d hope after 2 years). Story I could get is that this man had a syncopal episode. Received Narcan PTA by EMS and woke up. In the ED the patient adamantly denies heroin use–states he simply passed out. Luckily I got to him before EMS left, and EMS confirmed reports of bystanders stating opiate use.
Exam:
- Vitals: HR 120, RR 16, O2 96%, BP 80/45, T 98.0
- Gen: Fully A&O, drowsy
- CV: tachycardia
- Pulm: CTAB
- ABD: NT/ND
- Neuro: CN II-XII intact, motor intact, sensation intact, ambulates without difficulty to bathroom
My initial thought was that he may need some more narcan or that he received a longer acting opiate. The tachycardia was a wild card and didn’t make much sense with the picture. He remained afebrile and temp recheck, so I wasn’t thinking sepsis much at that time. At this point due to the tachycardia not making sense I ordered labs (and a tox for co-ingestants) and thought his BP/HR would improve with fluids.
I reassessed him after bolus #1 and #2 and neither HR or BP improved. Labs returned with an elevated WBC at 19.6. Opiates positive on top but otherwise were unremarkable. EKG sinus tachycardia. CXR and urine unremarkable. At this point even though I had no fever or source I felt compelled to initiate a septic workup and Lactate returned at 7.9.
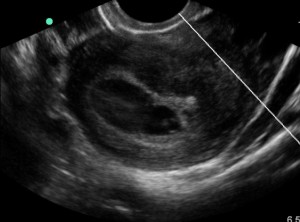
I was starting to get lost as why this guy was so unresponsive to fluids and O’Brien and I threw the USN to bedside at this point. Turns out he was in acute systolic failure with an ejection fraction of 11%. No history of CHF and also no signs of volume overload on exam except very mild pulm edema. Troponin peaked at 0.5.
He was admitted by cardiology while they trended his status. He went to the cath lab on hospital day 3 with clean coronary arteries. Ejection fraction improved to 60% by time of discharge. Talking with the team today they are still uncertain of the cause.
These are two cases of sick patients being in the holding area. Hopefully, it serves to remind everyone that any patient can be sick.
![Room9er ["Room Niner"]:](https://room9er.com/wp-content/uploads/2020/03/cropped-Screen-Shot-2020-03-08-at-3.16.16-PM.png)